
Commentary
Hollywood’s Harassment of the Soul
Gay men know harassment, too .


Michael Kearns (Photo courtesy Michael Kearns)
In the wake of the Harvey Weinstein travesty, many in the media want to know what the comparable gay story is. What homomogul has been unconscionably accosting male stars on the ascent, promising them an Oscar nomination in exchange for a “massage?”
There isn’t one.
I arrived in Hollywood in 1971, during that period when Weinstein “came of age.” Nearly five decades, and god-only-knows how many of those plus-size white bathrobes later, the King of Hollywood is without a throne.
“That was the culture then,” the disgraced Hollywood powerhouse explained to justify a list of immoralities and illegalities, like jerking off in front of his prey in random public places. Silly me, I thought the 70s culture was defined by Nixon in China and Bette at the baths; it never occurred to me that I could be wanking in line at the grocery store.
Performing in Tom Eyen’s The Dirtiest Show in Town (’72) was of “the culture then,” attracting a slew of entertainment heavyweights who came to oogle a bevy of mostly twentysomethings, strutting the stage au naturel, performing topical sketch material and elegantly choreographed orgies.
Allan Carr, the flaming manager-producer, attended opening night, outshining the likes of Merv Griffin (with a Gabor as an appendage), Cass Eliot, Christine Jorgenson, and Christopher Isherwood with Don Bachardy. Fully-clothed cast members segued their skilled seduction with audience members at a post-show party, setting our sights on which celebs might further our nascent careers. I chose Alan.
When I heard about the 2014 incident involving gay director Bryan Singer, accused of predatory behavior with boys in their late teens (aka minors) at house parties, I conjured the bygone days of Allan Carr’s notorious parties in which he deliberately mixed dozens of gay boys with the likes of Ann-Margret, Rod Stewart and Salvador Dali. While Carr and Singer hosted parties with an array of ambitious young men, the comparisons end there.
Or do they?
I was one of those boys, hungry to triumph in an overwhelmingly competitive and homophobic business. After three years at a prestigious acting school, I did not see myself as a boy-toy, in spite of the inevitable typecasting that resulted from how I looked.
After the Singer allegations (subsequently unsubstantiated and dropped), Time Magazine posited that “…the scandal has also thrown a spotlight on the places where the line between Hollywood networking and the casting couch is sometimes blurry, if not obscured altogether.”
And when the players are gay men on the casting couch, the blurriness gets blurrier. Let’s say that a closeted actor with heat and viable credits is threatened by homomogul in a robe (slate gray or barley beige). Because this scenario is played out in “the closet,” the victim wouldn’t say a peep, determinedly maintaining his straight persona.
Not identifying sexual predators because an actor can’t pry himself out of the closet is cowardly. Let the throngs of cowardly straight and gay Hollywood predators—from above-the-title stars to producers and directors with clout—squirm in silence while they await the ineluctable sound of sirens.
For hundreds of years, women in Hollywood have been bullied, derided, belittled, objectified, intimidated, brow-beaten, oppressed, persecuted and harassed; they are mad as hell and they aren’t going to take this anymore. These sheroes include the brave women who have taken on Cosby as well as everyday women everywhere—from all businesses and walks of life—who refuse to have their souls obliterated by narcissistic pigs.
Carr threw a lavish all-male party for his pal, Elton John, and invited the purportedly most gorgeous young men (not teenagers) in Hollywood who stood in an endless snaky line in order to meet and make an instantaneous impression on The Rockstar.
I had never felt so humiliated, knowing I would not be Elton’s trick for the night; not muscular enough, not blond enough, I was too tall, too soft, my voice was wrong, my face imperfect. I finally admitted the truth about myself: I was “a piece of shit.” Forget the acting credentials; forget my cherished friendships, forget my career accomplishments. I was of no value.
To suggest that perceiving oneself with such severe self-hatred leads to a rash of
debilitating behaviors doesn’t begin to describe what I, and too many of those other soulful party boys, would endure when the party ended.
Janice Min, former Editor of the Hollywood Reporter, told Time Magazine that the “predatory nature of Hollywood is young attractive people—largely female—putting themselves in front of men to be judged and appraised and chosen.”
Gay men also put “themselves in front of men to be judged and appraised and chosen.” Have you been to the Abbey?
I didn’t perceive that the Hunk Auction for Sir Elton could be deemed as sexual harassment. Yet I learned that a moment of extreme humiliation takes years—no, decades—to overcome.
Today, there are no excuses, in Hollywood or anywhere else for anyone—female, male, gay, straight, black, white—to have their soul harassed.
— Michael Kearns is a longtime theatre artist/activist, author and teacher. He is performing at Akbar in Silverlake on Oct. 22.

Commentary
Is Trump setting a trap for White House journalists at their big dinner?
White House Correspondents Association must do something to honor the free press

The old order is gone. Donald Trump didn’t just upset the apple cart of traditional rules and propriety – he set it on fire and laughed as his sycophants ushered his retreat into a fantasy gilded castle where he can be king for life.
Even beloved former First Lady Michelle Obama set aside her famous “we go high” approach to morally withered Republicans and, in the face of the obvious dangers to democracy Trump presented, urged Democrats to get politically practical before the 2024 elections.
“If we start feeling tired, if we start feeling that dread creeping back in, we’ve got to pick ourselves up, throw water on our faces, and do something,” Obama said.
Do something.
The grassroots chorus from “We the People” has grown louder and louder since regular, ordinary people took to the freezing, snow-covered streets of Minneapolis to protest the killing of two American citizens trying to protect their immigrant neighbors from militarized ICE agents. Recently, momentum from the massive No Kings rallies has shifted to local, regional, and state races as the critical midterm elections approach, and Democrats have been largely successful in their new “fight fire with fire” strategy.
But Trump seems obsessed with building his $400 million ballroom instead of doing something to help Republicans win elections, including sitting on an unspent $500 million war chest, while, as Alternet notes, his popularity steadily declines among once fierce loyalists.
“Even Fox News is now reporting Trump’s approval rating has plummeted to 33 percent [AP/NORC poll] over his foolish decision to send the US economy into a likely recession over his decision to fight an unnecessary and unprovoked war of aggression,” wrote David Pyne, a former America First Trump supporter and security expert who serves as a Deputy Director of National Operations for the Task Force on National and Homeland Security.

Meanwhile, Trump continues to stick it to the media, which he describes as the “enemy of the people.” That group now includes former conservative allies like Tucker Carlson, Megyn Kelly, Candace Owens, and Alex Jones, who he describes as “nut jobs” and “troublemakers” for criticizing him over the still-unexplained war in Iran.
Trump likes using his power to humiliate – especially women journalists of color – and retaliate against his enemies, a key tenet of the Authoritarian Playbook that organizations like Protect Democracy continue to update and explain.
“I say up front, openly, and proudly, that when I WIN the Presidency of the United States, they and others of the LameStream Media will be thoroughly scrutinized for their knowingly dishonest and corrupt coverage of people, things, and events. Why should NBC, or any other of the corrupt & dishonest media companies, be entitled to use the very valuable Airwaves of the USA, FREE? They are a true threat to Democracy and are, in fact, THE ENEMY OF THE PEOPLE! The Fake News Media should pay a big price for what they have done to our once great Country!” Trump’s post on Truth Social, Sept. 2023, before winning a second term in 2024.
The Authoritarian Playbook for 2025 explains: “A hallmark of any democracy is the freedom to criticize the government without fear of censorship or reprisal. Trump has promised — and has developed plans — to use the regulatory and administrative powers of government to force political loyalty; sow disinformation; and quash speech by journalists and media outlets, businesses, and other private citizens. These plans follow the measures used by Viktor Orbán in Hungary and other 21st-century autocrats to transform government power to serve the parochial interests of the ruler, not the broader public.”
Despite Trump’s support, Orban recently lost re-election, ending 16 years of “electoral autocracy.”
Trump and his administration also expanded attacks on the First Amendment, with the FBI investigating a New York Times reporter who wrote about the director Kash Patel using taxpayer-funded bureau personnel and resources to provide security for his girlfriend. The investigation included searching databases for information on reporter Elizabeth Williamson to see if she broke any federal stalking laws.
“The F.B.I.’s attempt to criminalize routine reporting is a blatant violation of Elizabeth’s First Amendment rights and another attempt by this administration to prevent journalists from scrutinizing its actions,” said Joseph Kahn, the executive editor of The Times. “It’s alarming. It’s unconstitutional. And it’s wrong.”
Interestingly, news of the Justice Department’s apparent retaliatory action leaked days before the White House Correspondents Association (WHCA) dinner on Saturday night, April 28. Trump’s acknowledgement of the WHCA invitation is like an obnoxious little boy sticking his tongue out.
“The White House Correspondents Association has asked me, very nicely, to be the Honoree at this year’s Dinner, a long and storied tradition since it began in 1924, under then President Calvin Coolidge. In honor of our Nation’s 250th Birthday, and the fact that these “Correspondents” now admit that I am truly one of the Greatest Presidents in the History of our Country, the G.O.A.T., according to many, it will be my Honor to accept their invitation, and work to make it the GREATEST, HOTTEST, and MOST SPECTACULAR DINNER, OF ANY KIND, EVER! Because the Press was extraordinarily bad to me, FAKE NEWS ALL, right from the beginning of my First Term, I boycotted the event, and never went as Honoree. However, I look forward to being with everyone this year. Hopefully, it will be something very Special. Thank you for your attention to this matter! President DONALD J. TRUMP,” he posted March 2 on Truth Social.
Some enraged journalists called for the fundraising dinner to be cancelled. Veteran ABC News journalists Ian Cameron and Lisa Stark had another idea: get colleagues to sign a public letter to WHCA urging them to do something to protest Trump’s authoritarian tactics.
“We first began thinking about this in late March, as it became clear the President would attend the dinner. We just felt we had to speak out about this,” former ABC News correspondent Lisa Stark told LGBTQ+ Freedom Fighters. “The WHCA dinner is held to celebrate the First Amendment and freedom of the press, and yet the guest of honor is the man who, along with his administration, has done everything possible to undermine freedom of the press and destroy trust in the press.”
The response has been overwhelming. After several days of outreach, the ad hoc group collected 414 signatures (including mine as a former journalist for CBS News/LGBTQ press), as well as six press/First Amendment organizations.
“It’s gratifying that so many former journalists see a threat to press freedom and want to speak out,” says Stark. “We know current journalists, those in the media trenches now, aren’t in a position to raise their voices. We feel an obligation to do so on their behalf. We can’t treat this as business as usual – these are not normal times.”
The petition cites 22 instances of Trump’s attacks on the press and First Amendment, not including the most recent involving the NY Times and updates on the Associated Press lawsuit.
“The collective weight of the administration’s actions — retaliatory access bans, coercive regulatory investigations, frivolous lawsuits against the press, defunding of public broadcasting, dismantling of international broadcasting, physical restrictions on journalists, personal verbal attacks on reporters, assaults on the media in official White House press releases and social media posts, the arrest of journalists, and the pardoning of those who committed violence against the press — represent the most systematic and comprehensive assault on freedom of the press by a sitting American president,” the petition reads, in part.
“We understand that some journalists plan to wear pocket handkerchiefs or lapel pins with the words of the First Amendment,” the petition says. “And continuing in that spirit, we believe the White House Correspondents Association should take stronger action by issuing – from the podium – a forceful defense of freedom of the press and condemnation of those who threaten that freedom, followed by a standing toast to the First Amendment and a pledge to continue upholding such a critical cornerstone of our democracy. Speak forcefully, in front of the man who seeks to undermine our country’s long tradition of an independent, strong, and free press.”
The petition concludes: “We also urge the WHCA to reaffirm, without equivocation, that freedom of the press is not a partisan issue and that the Association will not normalize this behavior but instead fight back against any officeholder who has waged systematic war against the journalists whose work the dinner celebrates.”
What now? The Daily Beast reports that “Donald Trump will launch a ‘revenge’ attack on the White House media when he confronts them in person at a Washington dinner on Saturday night—then flee before there can be revenge.”
Might the WHCA DJ play him off stage with Roy Orbison’s “Running Scared?”
But Trump will have cronies in the room who will turn his antics into memes about “crushing” the “lamestream media.” It’s an obvious ploy to excite Trump’s base.
In a scathing column, longtime journalist Margaret Sullivan notes that some media companies and bosses have gone from courtesy to courting, “inviting blatantly anti-press officials, including the defense secretary, Pete Hegseth, and the White House deputy chief of staff, Stephen Miller, to be guests at their tables, or (in the case of David Ellison, CEO of CBS News’s parent company) even holding a separate dinner to “honor” Trump. Paramount, the parent of CBS News, is said to have invited Brendan Carr to their table; he is the FCC chair who has made a mockery of what should be his independent and non-partisan role; appointed by Trump, he has come down clearly on the side of the president’s allies in consequential decisions – including those involving Paramount’s mergers with other media corporations.”
“It’s akin to a fire department inviting arsonists to a gathering aimed at celebrating firefighting,” Sullivan quotes Oliver Darcy as writing in his media newsletter, Status.
So, gala attendees, as the petition asks, Please Do Something!
This is all particularly jarring for LGBTQ+ journalists. Eric Schultz was the first out gay deputy White House press secretary to give briefings during the Obama administration. Then came the first Black lesbian, Karine Jean-Pierre, during the Biden administration, and the independent WHCA assigned a seat (shared with the Boston Globe) and rotating pool responsibilities to the LGBTQ+ Washington Blade, which still retains the privilege.
But for those of us who remember President Reagan’s Press Secretary Larry Speakes laughing and ridiculing White House reporters when he was asked about Reagan’s position on AIDS, being officially seated was a big deal. When CSPAN started broadcasting the dinner in 1993, we scanned every TV inch to see who might be wearing Red Ribbons to the “Nerd Prom,” who might be gay, and who we knew to be closeted – spinning President Clinton’s anti-gay Don’t Ask, Don’t Tell policy to favor anti-gay Democratic Sen. Sam Nunn.
And then there was the “Golden Age,” as the Washington Post described the gala in 2023. “There was the time Ellen DeGeneres, just days out of the closet, canoodled with new girlfriend Anne Heche right in front of Bill Clinton. The time George W. Bush goofed around with a George W. Bush impersonator. The time Barack Obama dunked on reality TV star Donald Trump to the rapturous shrieks of the media elite. What a time to be alive, and in attendance, at the White House Correspondents’ Association dinner!”
Last year, post-COVID, WHCA was headed by married Black gay Eugene Daniels, MSNBC’s Senior Washington Correspondent. The stars were the parade of journalists of color, mostly women, who served as co-hosts, presenters, honorees, and award winners.
Daniels addressed the missing orange man in the room. “We don’t only extend invites to the presidents who say they love journalists or who say they’re defenders of the First Amendment and a free press. We invite them to remind them that they should be,” Daniels said.
“When Thomas Jefferson wrote in 1786 that, ‘Our liberty depends on the freedom of the press and that cannot be limited without being lost,’ he and the other framers of the United States understood the danger unchecked power poses to the ideals and people of this nation,” he continued.
“We journalists are a lot of things,” Eugene Daniels said last year to a ballroom of 2,600 attendees. “What we are not is the enemy of the people, and what we are not is the enemy of the state….Every single day, journalists in this country face threats of intimidation, lawsuits, and violence. Those attacks are meant to do one thing: stop us from sharing the truth with the people…
“I want to leave you with the words of a trailblazing journalist, Ida B. Wells, ‘The way to right wrongs is to turn the light of truth upon them.’ Despite everything, I’m still optimistic about the power of what we do and more assured than ever of the importance of defending it. Everyone in this room can and should stand in the breach. Everyone can and should push for what we know is right. Everyone can and should stand up against government interference in a free press. And a promise I make to you is that the White House Correspondents Association, this board, will always defend your right to do your jobs.”
We’ll be watching CSPAN. Show us you mean it. Do something!
Read the full petition with signatories here.
This is a cross-post from Karen’s LGBTQ+ Freedom Fighters Substack.

A right does not need to be banned to be restricted. Sometimes it only needs to be made uncertain.
That is what emerges from a closer examination of adoption access for same-sex couples across different countries. There is no broad legal rollback. What appears instead is a more subtle pattern: rights that remain on paper but become fragile, conditional, and uneven in practice.
Italy provides a clear example.
Since 2023, under the government of Giorgia Meloni, administrative decisions have limited the automatic recognition of both mothers in female same-sex couples, particularly in cases involving assisted reproduction abroad. In practice, many families have been forced into additional legal proceedings to validate relationships already established.
At the same time, Italy has intensified its opposition to surrogacy, extending penalties even to those who pursue it outside the country. Human rights organizations have warned that these measures disproportionately affect LGBTQ+ families, particularly male couples.
The judiciary, however, has pushed back.
In 2025, the Constitutional Court ruled that a non-biological mother cannot be excluded from legal recognition when there is a shared parental project. It also removed a long-standing restriction that prevented single individuals from accessing international adoption.
Italy has not eliminated these rights. But it has made them unstable.
When a right depends on litigation, judicial timelines, or shifting interpretations, it is no longer fully guaranteed.
In the United States, the structure differs, but the outcome converges.
At the federal level, same-sex couples can adopt. Yet the system varies widely across states.
Data from the Movement Advancement Project show that while some states explicitly prohibit discrimination in adoption, others provide no clear protections. In several states, licensed agencies can refuse to work with same-sex couples based on religious objections.
Access, therefore, is shaped not only by law, but by geography, institutions, and applied standards.
Research from the Williams Institute further complicates the narrative. Same-sex couples adopt and foster children at higher rates than different-sex couples.
The contradiction is clear.
Child welfare is invoked, yet the pool of available families is reduced. Faith is cited, yet it is used as a filter within publicly funded systems.
The consequences are tangible
children remain longer in care
processes become more complex
families face unequal scrutiny
What is happening in Italy and the United States is not isolated. Across parts of Europe, conservative governments have advanced legal frameworks that reinforce traditional definitions of family while limiting recognition of diverse ones.
Adoption is not always addressed directly. But the impact accumulates.
Options are restricted while the language of protection is used to justify it.
There is no need to soften it.
This is not only a debate about family models. It is a decision about who is recognized as family and who must continue asking for permission.
That is not neutral.
It is political.
And when a right depends on where you live, who evaluates you, or how hard you are willing to fight for it, that right is already being weakened.
Commentary
Running loud & proud: Stephen Post brings energy, advocacy, and experience to the West Hollywood City Council race
West Hollywood City Council candidate Stephen Post shares his thoughts on the future of the City and his plans for it.

Last year on 4/20, I stood outside Pleasure Med in West Hollywood, surrounded by community, advocates, and organizers, hosting a cannabis justice event where Last Prisoner Project (LPP) was honored by the City of West Hollywood for helping clear more than 200,000 cannabis records across California.
This year, on 4/20, I’m running for West Hollywood City Council.
West Hollywood has always been more than just a city to me. It’s a symbol of what’s possible when people fight for dignity, visibility, and justice. As a queer person, I know firsthand how powerful it is to live in a place where you can hold your partner’s hand without fear, where your identity is not just accepted, but celebrated. But we can’t take that progress for granted, especially today with increasing attacks on our LGBTQ+ community. WeHo can’t wait for the next generation of bold ideas.
This evolution from advocate to candidate is an example of how I have been translating queer joy into queer power.
Last year, I helped coordinate the Loud & Proud campaign in partnership with Culture Machine and LPP, which was rooted in a simple but urgent truth: the LGBTQ+ rights movement and cannabis justice movement are deeply intertwined. Both were born out of resistance. Both have been criminalized. And both are still fighting for full equity and inclusion.
My work with the Last Prisoner Project has taken me across the country organizing, advocating, and building coalitions to free those still incarcerated for cannabis offenses. I’ve sat with families who have lost decades with their loved ones. I’ve worked alongside directly impacted individuals who turned their pain into purpose. And I’ve seen what can happen when policy finally catches up with people: healing, restoration, and hope.
But advocacy alone isn’t enough. We need leaders inside government who understand these issues not as abstract policies, but as lived realities.
That’s where this campaign comes in.
West Hollywood is at a crossroads. We are a city that has led on LGBTQ+ rights, on tenant protections, and on cannabis legalization, but leadership means continuing to evolve. It means asking hard questions: How do we ensure our cannabis industry remains equitable and locally beneficial? How do we protect renters in a city where housing costs continue to rise? How do we preserve the cultural vibrancy that makes West Hollywood the creative city?
I believe the answers start with community.
We need to strengthen our local cannabis economy while advocating for state and federal reforms that allow our businesses to thrive. We need to protect and expand rent stabilization tools so that longtime residents aren’t priced out of the community they helped build. And we need to think bigger about what West Hollywood can be. From creating a world-class, large-scale cannabis festival that rivals our iconic Pride celebrations, to investing in small businesses, nightlife, and the creative economy that defines our city.
This is the energy I bring, but this campaign is also about experience.
I’ve spent years organizing at the intersection of policy and people. Whether it’s working with local leaders, engaging state officials, or building national coalitions, I know how to move ideas into action. I know how to bring people to the table. And I know that real change requires both urgency and persistence.
Running for office, especially as a young, queer advocate, comes with its own set of challenges. But West Hollywood has never been a city that backs down from a challenge. We are a community built by people who refused to be silent, who refused to be invisible, who refused to accept the status quo. I am fighting for a West Hollywood where we honor this history, while shepherding a future that works for everybody.
I’m Stephen Post, and I am running loud and proud to be your next West Hollywood City Council member. Join me by visiting post4weho.com or supporting with a donation here.
Commentary
When “election integrity” becomes voter suppression
Trump’s executive order would not stop fraud. It could stop eligible Americans,
including many LGBTQ+ voters, from casting a ballot.

On March 31, 2026, President Donald Trump signed Executive Order 14399 entitled: “Ensuring Citizenship Verification and Integrity in Federal Elections.” Who could oppose election integrity?
That is precisely why Americans should read beyond the title.
Beneath the falsely reassuring rhetoric, EO 14399 is an unprecedented attempt to place new federal barriers between millions of Americans and the ballot box. It doesn’t just tinker at the margins. It tries to rewire the entire machinery of mail-in voting — fast, through agencies that were never built for this job, on a timeline that virtually guarantees error.
What the Order Actually Does
The order does three major things. First, it directs the Department of Homeland Security — working through U.S. Citizenship and Immigration Services and the Social Security Administration — to build state-by-state “State Citizenship Lists” from federal databases, and transmit those lists to state election officials at least 60 days before every federal election. DHS must stand up this entire infrastructure within 90 days.
Second — and this is the part that should alarm every voter — it directs the U.S. Postal Service to issue rules within 120 days that would make USPS a gatekeeper for ballot delivery. Under the order, USPS “shall not transmit” mail-in or absentee ballots unless a voter is enrolled on a federally mandated state-specific participation list. Miss the list, miss your ballot.
Third, it escalates enforcement pressure by directing the Department of Justice to prioritize prosecutions of officials involved in distributing ballots to anyone deemed “ineligible,” and threatens to withhold federal funds from states that don’t comply.
A Solution in Search of a Problem
Supporters say this is simply about ensuring only citizens vote. But noncitizen voting in federal elections is already illegal — and federal criminal statutes, including 18 U.S.C. § 611 (voting by aliens) and 52 U.S.C. § 20511 (criminal penalties under the National Voter Registration Act), already exist to prosecute it. If the goal were simply to enforce existing law, there would be no need to rebuild the entire mail-in voting infrastructure from scratch.
The Brookings Institution has analyzed mail-in voting fraud and found it exceedingly rare, while documenting the significant access advantages mail-in voting provides — especially for working people, seniors, and disabled voters. You don’t respond to a low-incidence problem by building a nationalized gate that creates a far higher-incidence exclusion problem.
The Database Problem Is Real
Here is what gets lost in the political noise: federal databases are deeply imperfect. They contain gaps, mismatches, and outdated information — especially for people who have moved, changed names, naturalized, or had records created in different eras.
A joint investigation by ProPublica and The Texas Tribune found that SAVE — the federal immigration-status verification system at the heart of this order — has repeatedly produced false flags, including widespread misidentification of citizens born outside the United States. The U.S. Government Accountability Office has likewise flagged SAVE’s accuracy problems and the urgent need for meaningful error-correction mechanisms. Those safeguards don’t exist yet. This order would tie voting access to that flawed system anyway.
A misspelled surname. A missing hyphen. A record that didn’t update when someone naturalized. In most settings, those are fixable administrative errors. In elections — where deadlines are real, and the burden falls on the voter — they become functional disenfranchisement.
Why LGBTQ+ Voters Are Especially at Risk
These barriers don’t fall evenly. They fall hardest on people whose lives are more likely to be out of sync with “official” records. And for LGBTQ+ Americans, that is not a hypothetical concern.
Consider transgender voters. The Williams Institute estimates that in 2024, more than 200,000 voting-eligible transgender people lacked ID documents fully reflecting their correct name and gender. EO 14399 is not a voter-ID-at-the-polls order — it is a record-matching order. And record-matching systems are precisely where mismatches become denials. A transgender voter may have updated their driver’s license but not their Social Security record. A former name in an older federal database could be enough to leave them off the list entirely.
And consider housing instability. The Williams Institute also reports higher rates of recent homelessness among transgender adults than among cisgender peers — and housing instability is one of the most common ways people fall out of sync with official records. When ballot delivery is driven by centralized lists and rigid deadlines, people who have moved, rebuilt, or stabilized after disruption are most likely to be missed.
The same risk extends to anyone whose life doesn’t fit neatly into a database: the college student who just moved apartments, the senior citizen who votes by mail because standing in line for hours is physically difficult, the veteran stationed overseas, the lesbian couple who recently changed their last names, the working parent who cannot take half a day off to vote in person.
What This Means for California
California has built one of the most accessible voting systems in the country. Every active registered voter receives a ballot by mail. Californians can vote from home, return ballots through drop boxes, or vote early in person. That system has meaningfully expanded participation — especially among young people, working people, disabled people, and communities historically excluded from politics.
EO 14399 strikes directly at that model. If implemented, it would allow Washington politicians and federal agencies to decide whether Californians are “eligible enough” to receive the ballot they have long been entitled to.
Why the Courts Are Already Pushing Back
The order is already in court. A coalition of Democratic-led states sued in federal court in Boston to block it, arguing it violates the Constitution and interferes with state election systems. The ACLU and partner organizations filed a separate challenge. Legal scholars across the political spectrum have concluded the order is likely unconstitutional.
The reason is structural. Under the Constitution’s Elections Clause, states — not the President — administer the times, places, and manner of elections, subject to congressional override. The President cannot unilaterally redesign election administration and mail services through executive order. Congress built USPS as an independent establishment (39 U.S.C. § 201) precisely to keep universal mail service from becoming a political lever. Its basic statutory function is to “bind the Nation together” — not to police ballot eligibility.
But Americans should not take comfort in assuming the courts will save us. Even if this order is ultimately struck down, it serves another purpose: creating confusion, fear, and uncertainty around voting. That confusion alone can suppress turnout. If voters begin to wonder whether they are still registered, whether they will receive a ballot, or whether some technical mistake will disqualify them, many will simply give up. That is the point.
What We Should Do
The LGBTQ+ community knows better than most how rights are eroded: rarely all at once, more often piece by piece, under the guise of procedure, bureaucracy, or “integrity.”
Treat EO 14399 for what it is: a power play falsely packaged as integrity. Demand that courts enforce the constitutional boundary lines. Demand that Congress do its job in the open — if election rules are going to change, they should change through legislation, not executive improvisation. Demand transparency from agencies about data quality, error rates, and correction processes before a single election system is forced onto the public. And support the organizations litigating this.
And if you are registered to vote: check your registration, confirm your mailing address, and make sure your records are current. Because the most powerful answer to efforts to make voting harder is to vote anyway.
Real election integrity means making sure every eligible American can cast a ballot and have it counted. What EO 14399 builds is something else: a system designed to treat eligible voters as suspects, and to make participation conditional on perfect paperwork. If we normalize that, IT WON’T STOP HERE.
Edward Campbell is a Los Angeles-based attorney, LGBTQ advocate, and civil rights activist with extensive experience in affordable housing finance and preservation. He has worked on housing policy at the federal, state, and local levels and is a longtime advocate for racial equity and democratic institutions.
Let’s face it, whether you were raised Christian, Muslim, or Mormon, there is a fundamental friction between religion and queer identity. This is one of the pillars of homophobia, pitting religion against queer people. But does this rob us of healthy spiritual lives?
We are living in crazy times where we are witnessing true evils in the world. Whether it’s war, genocide, famine, or TLC’s MAGA ties (RIP Chilli). The Supreme Court ruled against Colorado’s law banning conversion therapy, citing religious freedoms. Is the answer for us as queer people to be free to believe?
It’s starting to feel like we’re in a spiritual war. So how do we arm ourselves? How can we heal the sense of alienation from spirituality we got from hateful sermons, homophobic religious zealots in our family, or just plain ignorance? That way, these issues with religion don’t rob us of healthy spiritual lives. After all, if you don’t believe in anything, you’ll fall for anything.
It’s understandable we might reject our religions of origin, growing up being confronted with rejection by our families, communities, or a religion that preaches issues with something we cannot change. To quote The Book of Gaga, we were born this way.
And yet, without thriving spiritual lives, we can end up susceptible to issues like addiction, depression, or questionable moral quandaries. It begs the question: Is this religious trauma something we can heal?
Whether it’s a queer-friendly church, the wonders of witchcraft, or a thriving meditation practice, honoring this area of our lives can be so transformative. I define a spiritual life as anything that encompasses all of the mental, emotional, physical, and holistic concepts that govern our lives. Or anything that doesn’t quite fit into it, like what happens when we die? Does our attitude influence the world around us? Aliens?
Spirituality is half of what we fundamentally know to be true, i.e., our values, morals, our intuition, and making peace with what we’ll never understand and control.
If you think about it, it makes sense. We need to be able to give our ego a rest to deal with the myriad of things that are outside of our control. Our questioning of religion is not that off base, considering how many people live with religions that preach peace and love but allow war, that argue against queer sex but ignore the sex crimes of religious and political leaders. They argue for the lives of theoretical children and ignore starving and abused children. That being said, the issue is with them and not their faith.
I grew up going to Catholic school for 14 years. It wasn’t until I found myself spiritually questioning that I went out and explored other religions, spiritual practices, and fundamentally learned firsthand the definition of all the stuff that was preached at me growing up: joy, grace, charity, and even prayer.
I’d argue that half the people out there say all these prayers and don’t even know what they mean. But what are we queer people to do? Atheism isn’t the clapback people think it is. If we don’t fundamentally heal the trauma of rejection, persecution, and bullying we face from our religious pasts, it stays with us. That unhealed trauma still exists even if you say there’s nothing out there. If we don’t heal the wound, we are just as faulty as the people who persecute us.
Instead, I think it’s incumbent on us as queer people to figure out what we do believe, value, and how we define love to be more whole and live fuller lives.
Whether you find value in Buddhist traditions, meditate by chanting or breathwork, or even if you just worship at the altar of the Law of Attraction, we need something larger than ourselves to capture all the unknowns and heal what we can’t heal ourselves.
I’ve always struggled reconciling the religion that supported colonialism and slavery. So I explored some of the African and indigenous traditions that still survived in my culture.
At the end of the day, all of the religious traditions out there have something right. If not, they wouldn’t be able to get practitioners. The fundamental issue is the people, not the religion.
My hot take is this. If we find something that we believe in that makes us better people, helps us separate from our ego and our primal fears to make more embodied choices, I think that that’s something of value.
As queer people, no matter how resilient, powerful, and fabulous we are, we deserve peace of mind, freedom of spirit, and the belief in something that has our back. By finding a way to heal what religion has taken away from us: community, morality, and a spiritual life, that’s how we really heal the religious trauma, rather than just acting like none of it is worth retaining.
After all, at the end of the day, if you strip away the unhealed egos and toxic hatred of many religions, they are simply a couple of ideal rules to live by and a couple of spiritual tips and tricks for how to navigate the world.
Ironically, we are in a position to choose what works for us, and given our existence in the fringes and the middle space, we can see what’s bullshit and what’s fundamentally true for us. There’s a certain magic we can experience as queer people, and we shouldn’t let our pasts rob us of that.
Christian Cintron is a jack-of-all-trades and master of fun. He’s a writer, comedian, actor, and spiritualist. He created Stand Up 4 Your Power, a program that teaches self-empowerment through stand-up comedy.
Commentary
As No Kings momentum shifts to midterm elections, beware of expectation traps
LA County Supervisor Lindsey Horvath is not taking reelection for granted

It’s a lot. And that’s what the diverse No Kings coalition promoted in organizing their historic March 28 non-violent protest. Regardless of political party or ideology, everyone was welcome to bring their issues and rally around the central constitutional concept that America has no kings, no one is above the law, and “We the People” hold the power, not some spray-painted, man-child wanna-be dictator.
More than 8 million people showed up for the nation’s third No Kings protests with 3,300 anti-authoritarian rallies in all 50 states and on every continent (except Antarctica), connecting with neighbors and strangers in venues large and small, demonstrating that resistance is not futile, as Donald Trump and his ruthless, Borg-like Christian National cult of storm troopers want the world and American voters to believe.
On Friday, April 3, No Kings will host a debriefing on “Where We’re Going.” The No Kings website also features suggestions for continued participation.
Motivating concerns abound as young people struggle with nihilism and Vietnam War-era Baby Boomers like former Vice President Al Gore still deliver dire warnings about climate change and the planet’s future.
But the immediate concern is real. “The President and his advisors are in the midst of what I believe is the greatest geopolitical disaster in the history of our country,” Brig. Gen. Steve Anderson (US Army, retired) told MS Now about the impact of Trump’s war with Iran.
The scandalous lack of promised transparency with the Epstein files and the costly, chaotic, unexplained war in Iran have awakened MAGA supporters. Giuseppe Palazzolo from Staten Island told MS Now he is pissed off because Trump promised no more wars. Now, “we’re knee deep in this illegal war and we’re closer to catastrophe than ever before. I feel so betrayed,” Palazzolo said. “It’s one lie after another. It’s like dominos falling on top of each other….This isn’t about right or wrong. It’s about truth versus deception.”
Wednesday, April 1, is a head-spinner. SCOTUS alarmingly considered the constitutionality of Trump’s January 20, 2025 executive order ending birthright citizenship, followed by NASA’s Artemis 2 liftoff to the moon. Trump ends the day with a talk to the nation about Iran. April Fools.
Meanwhile, normality keeps unraveling – such as SCOTUS’s 8-1 decision to allow so-called “conversion therapy” for LGBTQ+ kids. The debunked religious-based “reparative” talk therapy was outlawed in California on October 1, 2012. The bill’s sponsor, then-Calif. State Sen. Ted Lieu, called it psychological child abuse. Gov. Jerry Brown said the therapies “have no basis in science or medicine and they will now be relegated to the dustbin of quackery.” Now-Rep. Lieu and the Congressional Equality Caucus filed an amicus brief with SCOTUS opposing the challenge.
“This ruling is a profound failure of both logic and moral responsibility that confuses ‘free speech’ with ‘false speech’,” Wayne Besen, Executive Director of Truth Wins Out, said in his strong condemnation of the decision.

As attention shifts to the midterm elections, the No King protests will be remembered for joy, humor, empathy, love, and unity, following the neighbor-helping-neighbor example Minnesotans set protecting their undocumented neighbors and resisting the ICE madness that murdered two American citizens – lesbian poet and mother Renee Good and ICU nurse Alex Pretti – as they caused “good trouble.”
Actor/anti-Vietnam War activist Jane Fonda, 88, read a letter from Renee’s widow, Becca , at the St. Paul rally.
“I am so heartbroken. I miss my wife. The world now knows that my wife sparkled with sunshine and shone with kindness that was unmatched. We were robbed of an incredible human. It has made people pause, take a breath, and choose sides. We choose the side of love,” Becca said in the letter. “I feel it’s my responsibility to send a message that hate has divided us and destroyed so many lives and families, but we can choose something else. We can choose radical kindness.”
California turned out – including in Orange County’s Anaheim and conservative districts like Huntington Beach, where MAGA culture warriors wield electoral power, and islands of Democrats like Stockton, where trans flags flew on the frontlines. Indeed, Stockton is a prime example of assumption-busting: though surrounded by ruby red Republicans, this blue gem elected out Susan Talamantes Eggman to serve on the Stockton City Council in 2005 and then in the State Legislature until her retirement in 2024.
Individuals like Ilka, 52, turned out, too, protesting in downtown LA dressed as the Statue of Liberty. “I’m German, and the similarities are really striking to what happened in Germany in the 1930s,” she told the LA Daily News. “Same rhetoric, same mental attitude, same idea, same way of thinking. And so it’s really scary, and it’s really serious to me.”

Out attorney and former West Hollywood mayor/city councilmember John Duran, 66, connected historical dots at the No Kings rally in West Hollywood.
“I wear this [ACT UP] tee shirt proudly. It says ‘Silence = Death’ because we learned a very powerful lesson – that if we were silent in the face of oppression and fascism, it would surely mean our deaths. Instead, we showed up, we laid down in the streets, we protested, we ACTED UP, and we changed the world,” Duran said. “And so now, here you are. And here we all are in the year 2026. You and I were meant to be here now, at this period in time, to decide whether the American Dream persists or whether it is eliminated by those same forces that raise their head every 10 or 20 years.”

Meanwhile, Trump is obsessed with voter suppression.
“Voter fraud conspiracies are like methamphetamine running through MAGA veins, stirring up equal parts passion and paranoia,” writes LA Times columnist Anita Chabria. “President Trump, of course, is the king pusher of this particular addiction, pathologically certain he won the 2020 presidential election (he did not). In his second term, and in advance of the November election, Trump has supercharged voter fraud lies; installed election deniers in key positions; and is attempting through the so-called SAVE America Act to disenfranchise poor and female voters.”
On Tuesday, March 31, Trump signed an executive order calling on Homeland Security and the Social Security Administration to develop a nationwide list of verified eligible voters, bar the Postal Service from sending absentee ballots to people not on state-approved lists, and track envelopes. Experts say this is wildly unconstitutional and plan democracy-saving lawsuits. A showdown is ahead.
But visually, casual Californians may be intrigued by GOP Riverside County Sheriff Chad Bianco’s headline-grabbing stunts about voter fraud as he angles to become one of two Republicans in the June “jungle primaries” that decide the midterm runoff for Governor of California.
This may be a trap of voter expectation. Newsweek reported that since Trump returned to office, “Democrats have flipped over two dozen seats in special and state legislative elections nationwide” – including in Trump’s own Mar-a-Lago district – “a string of wins that has boosted the party’s outlook ahead of the 2026 midterms.”
No Kings also boosted a sense of Democratic inevitability. But great expectations are often undermined by unintended consequences.
Amy Walter, the respected out editor-in-chief of the Cook Political Report, delivered a warning, analyzing “How Predictive Are Special Elections?
“While Democrats are running strong in special elections, the generic ballot measure in national polls suggests a more modest advantage for Democrats — around six points,” Walters writes. “What’s more, media attention and campaign spending will be exponentially higher in November, which will generate a much different electorate than in low-turnout special elections that attract only the most highly activated voters.”
Then there’s this era’s version of the “Bradley effect” where voters tell pollsters what they think pollsters want to hear instead of how they really intend to vote, thus skewing data everyone relies on.
Social media and Trump’s constant blizzard of news often block information, even for pros. The New York Times LA-based political reporter Jennifer Medina wrote in: “Why There’s a Chance California Elects a Republican Governor:” “California — the state with the largest population, the biggest economy, and some of the country’s most powerful politicians — is electing a new governor this year. If that’s news to you, you’re not alone; even some California voters seem a bit unaware,” apparently including Medina, who writes that she called her Sacramento colleague to get filled in.
So who’s informing the electorate about state and local elections? Who’s fact-checking the distorted perceptions and propaganda?
Consider LA County Third District Supervisor Lindsey Horvath’s reelection, for instance. Lindsey Horvath’s district stretches from the Ventura County line to Santa Monica and Hollywood to Sylmar and San Fernando, with more than 2 million people, including me, in West Hollywood.
Lindsey and Fifth District Supervisor Kathryn Barger were on TV and other news outlets around the clock during the devastating wildfires last year, and their websites have a lot of resources.

Lindsey – who succeeded LGBTQ+ icon Sheila Kuehl as Supervisor – mixed empathy and compassion in reading the names of the dead before barely containing herself, questioning contractors and county leadership after an LA Times investigation into an After Action Report.
Lindsey also went on CNN’s “The Story is with Elex Michaelson” to discuss the one-year anniversary of the fires with the former FOX 11 LA anchor, telling him, “answers shouldn’t be watered down.” On March 17, the Board approved Lindsey’s motion to coordinate wildlife prevention among the patchwork of federal, state, county, and local agencies, plus private landowners across the Santa Monica Mountains, where 23,000 acres were burned during the 2025 fires.
But after an Aug. 2025 interview with LA Times Studio about the fires and what comes next, one commenter said: “Linsdsey is all talk, no action.” After a story in CityWatchLA, a commenter wrote: “Lindsey is the Queen of Self-Promotion, campaigning 24/7 and often coming off as quite obnoxious in the process.” One small business owner on Instagram complained about Lindsey’s proposal for rent relief.

Snark aside, after deciding to run for reelection instead of running against LA Mayor Karen Bass, Lindsey drew three Republican opponents – one of whom is a Calabasas real estate agent, Tonia Arey, whose “Facts about Lindsey” cites “Lindsey Horvath’s Record of Extremism,” promising “receipts to show it.” Well, not really.
Arey says the “Pacific Palisades fire and its aftermath were a breaking point for me.” But “protesting from the outside wasn’t enough—we needed leadership from within the system…it’s time for a change.”
Here’s another expectation trap. Though Arey is an unknown with no record of governance, Third District voters cannot assume Lindsey’s reelection is a done deal. This year, AHF’s Housing Is A Human Right division has no rent control measure on the ballot, so the big real estate corporations that killed two previous campaigns have money to spend. Additionally, former LA County Sheriff Alex Villanueva, who is running for his old job, endorsed Arey and may emulate Riverside’s Bianco by pulling political stunts.
Most importantly, Democrats must stop thinking everyone agrees with them. No. This is a new era. There is no unscrambling the egg Trump broke. Politically tetherless 15-year-olds watched Trump come down that escalator and give them permission to be racist. They found Charlie Kirk and White Supremacy/Christian Nationalism, sexism, and transphobia. They don’t know George Orwell. They are more ideologically bent online than old school partisans and more likely to prank a pollster than tell their truth. And at 26 today, they do not trust Democrats who throw their best supporters under the bus.
Young people and deflated elders may believe evidence of positive change, however. And Lindsey Horvath has done that with Measure G – the governance reform that Supervisors and others have promised and studied for decades.
The respected political outlet Capitol Weekly wrote a 5,000+ word anatomy of how “change agent” Lindsey Horvath passed Measure G after so many other attempts failed.
“That was the origin of Measure G, the revolutionary ballot measure approved by Angelenos in November 2024 that reshaped the nation’s most populated county by expanding the board of supervisors from five to nine members, making the county executive an elected official, and created a county ethics commission,” Brian Joseph wrote for his October 13, 2025, post.
“The measure represents not only one of the most significant governance reforms in California history, but also a breakthrough in Los Angeles County political gridlock, where changes of this nature had been discussed ad nauseam but always failed.
Reform of this gravity and consequence likely would rank as a crowning achievement for many lifelong, career politicians. Horvath pulled it off after just her first two years in big-time politics,” Joseph reported.

In a wide-ranging conversation, Lindsey talked extensively about Measure G, about what’s being done to prevent fires and help the victims and survivors of last year’s horrific catastrophe, as well as wanting to “earn that title of ally” to her West Hollywood-based LGBTQ+ community.
And, while she’s keenly aware that the Third District “has historically been very proudly blue, very proudly progressive and pragmatically progressive,” Lindsey says, “I don’t take anything for granted.”

“I’m running for another term because we have begun very important transformational work in the county that I do not want to step away from,” Lindsey says. “We will not abandon anyone – no matter how hard it gets.”
Check out Karen’s candid chat with Lindsey Horvath.
Karen Ocamb’s commentary is cross-posted from her Substack LGBTQ+ Freedom Fighters.
Commentary
LA Metro should approve the San Vicente-Fairfax route for the K Line Northern Extension without delay
As Angelenos wait, Metro is gearing up for another monumental decision about one of its next major projects coming to Los Angeles—one that may be even more transformative for how our region moves.

By: West Hollywood Mayor John Heilman, West Hollywood Councilmember Chelsea Lee Byers, and Congresswoman Laura Friedman
After a decade of construction, Metro’s D Line extension along Wilshire is about to open. Fast, efficient, and affordable rail service will whisk Angelenos to iconic destinations, making life better not just for visitors, but also for residents and commuters, too. As Angelenos wait, Metro is gearing up for another monumental decision about one of its next major projects coming to Los Angeles—one that may be even more transformative for how our region moves.
Metro is deciding between three routes for the K Line Northern Extension. The best option is the San Vicente-Fairfax route, which will connect the Hollywood Bowl, West Hollywood, Cedars-Sinai Medical Center, the Beverly Center, the Grove and Farmer’s Market, the Crenshaw District, Leimert Park, the South Bay, and LAX all on one line. This new north-south line also links up to the D and E Lines, allowing for easy transfers to UCLA, Santa Monica, Koreatown, and Downtown LA. All of this will take cars off the road, easing congestion and freeing up parking spaces.
Metro’s Board of Directors will vote on this project on March 18th and 26th, and their own staff recommends the San Vicente-Fairfax route because it will move the most riders and connect them to all the major destinations and job centers in this area. Metro should approve it without delay. On the day it opens, this new extension will be one of the busiest rail lines in the country, because it will serve so many people who currently don’t have access to reliable rapid transit.
Imagine getting to the Grove, WeHo’s Rainbow District, and the Hollywood Bowl—without all the traffic. The San Vicente-Fairfax route is the one choice to serve all these destinations. These are places that residents, commuters, and visitors all want to reach. Every time Metro has asked the public, the answer has been clear: overwhelming support to build this route and build it faster. The most recent comment period was no different.
The West Hollywood City Council has already proposed an approach to deliver part of the investment needed to make this plan a reality without raising anyone’s taxes. City analysis showed that an Enhanced Infrastructure Financing District (EIFD) in West Hollywood could generate more than $2 billion over 75 years, with the potential for a similar contribution from the County. This would be an unprecedented commitment from a local City, and a first in Southern California for a project of this size, but it also only makes sense if most WeHo residents are directly served by the San Vicente-Fairfax route. It is this unprecedented local investment that makes a project like the K Line Northern Extension possible in our lifetimes.
We’re excited about what this project will mean for our neighborhoods, but it will be transformational for much more than just West Hollywood and residents living directly along the new line. It will give more people more affordable options to move around the region and open up new mobility options for seniors and students.
Like the Regional Connector-linked Metro lines downtown, the K Line Northern Extension will provide a new north-south connection linking Metro’s east-west B, C, D, and E Lines with the new K line and the upcoming LAX people mover. Today, Metro’s rail network radiates out from downtown, forcing riders to travel out of their way to transfer or skip transit altogether. The K Line Northern Extension will change that by connecting Metro’s east-west rail lines and allowing riders to travel across the city without detouring through downtown. Traveling from the South Bay or the Valley to work in Century City or Westwood? This line will make high-quality transit a viable option for countless trips like those, ensuring that transit is more realistic for everyone.
The San Vicente-Fairfax route will link communities from Torrance to North Hollywood to job centers like Cedars-Sinai and Hollywood and put over 125,000 jobs within a short walk of new stations. Access like that is unprecedented—and it shows in Metro’s ridership estimates: The San Vicente Fairfax route will likely serve 100,000 daily trips—making it one of the busiest light rail lines in the entire country. This route will also better connect communities along the existing K Line to jobs and services they already rely on, as well as more of the opportunities and resources that might currently be out of reach.
With more riders, more jobs, more destinations, more opportunity, and a clearer path towards implementation, the choice is simple: the San Vicente-Fairfax route for Metro’s K Line Northern Extension. Let’s finish the line!
COMMENTARY
Who gets to vote? The SAVE Act and what it means for LGBTQ Americans
The real issue with the SAVE Act is not simply what the law says. It is how it will function in practice — and who will bear the burden.
At its core, democracy depends on a simple premise: if you are eligible to vote, you should be able to do so. The right to vote in the United States has never been just about who is legally eligible. It has always been about who can realistically access the ballot.
The proposed Safeguard American Voter Eligibility (SAVE) Act puts that premise at risk — and for LGBTQ Americans, particularly transgender and nonbinary individuals, the threat is direct and concrete.
The SAVE Act would require Americans to provide documentary proof of U.S. citizenship — such as a passport or birth certificate — when registering to vote in federal elections. Supporters argue this is a necessary step to protect election integrity.
But the real issue is not simply what the law says. It is how it will function in practice — and who will bear the burden.
Under current federal law, eligible voters can register by attesting to their citizenship under penalty of perjury. The SAVE Act would replace that system with a documentation requirement.
That may sound like a technical adjustment. It is not.
It represents a fundamental shift — from a system where the government verifies eligibility, to one where individuals must produce specific documents to prove it. And not all voters are equally positioned to meet that requirement.
For transgender Americans, identity documents are often not consistent across systems. A person may have legally changed their name but not updated all records. Their birth certificate may not reflect their current identity. Their passport, driver’s license, and Social Security record may not fully align.
Updating these documents is not always straightforward. In some states, it requires navigating complex legal processes. In others, it may be restricted altogether.
None of this changes a person’s eligibility to vote. But under the SAVE Act, it could determine whether they are able to register — and whether their registration is accepted. This is not a hypothetical concern. It reflects the everyday reality of navigating identity systems that were not designed with LGBTQ people in mind.
Supporters of the SAVE Act emphasize that the law applies equally to everyone. Formally, that is true. But equal rules do not guarantee equal access.
For voters with straightforward documentation, the requirement may be manageable. For those whose records are inconsistent or difficult to obtain, it creates additional hurdles — delays, rejections, and uncertainty. That is how neutral policy produces unequal outcomes. And in the context of voting, those outcomes matter.
The SAVE Act may not result in voters being turned away in large numbers on Election Day. That is not how these systems typically work. The risk is more subtle — and more systemic. Registration applications get delayed or rejected. Confusion about what documentation is required discourages people from trying. Voters give up rather than navigate a bureaucratic maze. For LGBTQ Americans, a system where friction can become total exclusion.
For LGBTQ Americans already navigating barriers in healthcare, housing, employment, and basic legal recognition, this is one more arena where that friction compounds. Over time, that erosion of participation weakens the democratic process itself.
Election security is a legitimate concern. Policy should be grounded in evidence, not self-serving conspiracy theories. Federal law already prohibits noncitizens from voting, and there is no credible evidence of widespread noncitizen voting in federal elections. Existing safeguards — verification systems, database checks, and legal penalties — already address that risk.
The SAVE Act proposes a sweeping change to address a problem without evidence. In doing so, it risks disenfranchising large numbers of LGBTQ Americans, as well as women, Black, Indigenous, and people of color, low-income Americans, and young voters — the communities that have historically faced the greatest barriers at the ballot box.
For LGBTQ Americans, the SAVE Act is not just about election policy. It is about whether systems account for lived reality — or ignore it. The right to vote should not depend on whether your paperwork is perfectly aligned across multiple bureaucracies. It should depend on whether you are eligible.
That is the standard a functioning democracy should meet. And then it should make the act of voting as easy as possible for all eligible Americans.
The SAVE Act does none of that. Because the question it answers is not how we make elections more secure. It is, in practice, how we keep Americans from voting.

Edward Campbell is a Los Angeles-based attorney, LGBTQ advocate, and civil rights activist with extensive experience in affordable housing finance and preservation. He has worked on housing policy at the federal, state, and local levels and is a longtime advocate for racial equity and democratic institutions
Commentary
The harms of our leaders do not erase our movements and voices
The Blade sits with the exposed harms of late labor champion Cesar Chavez, and how collective reckoning cannot sacrifice victim testimonies.
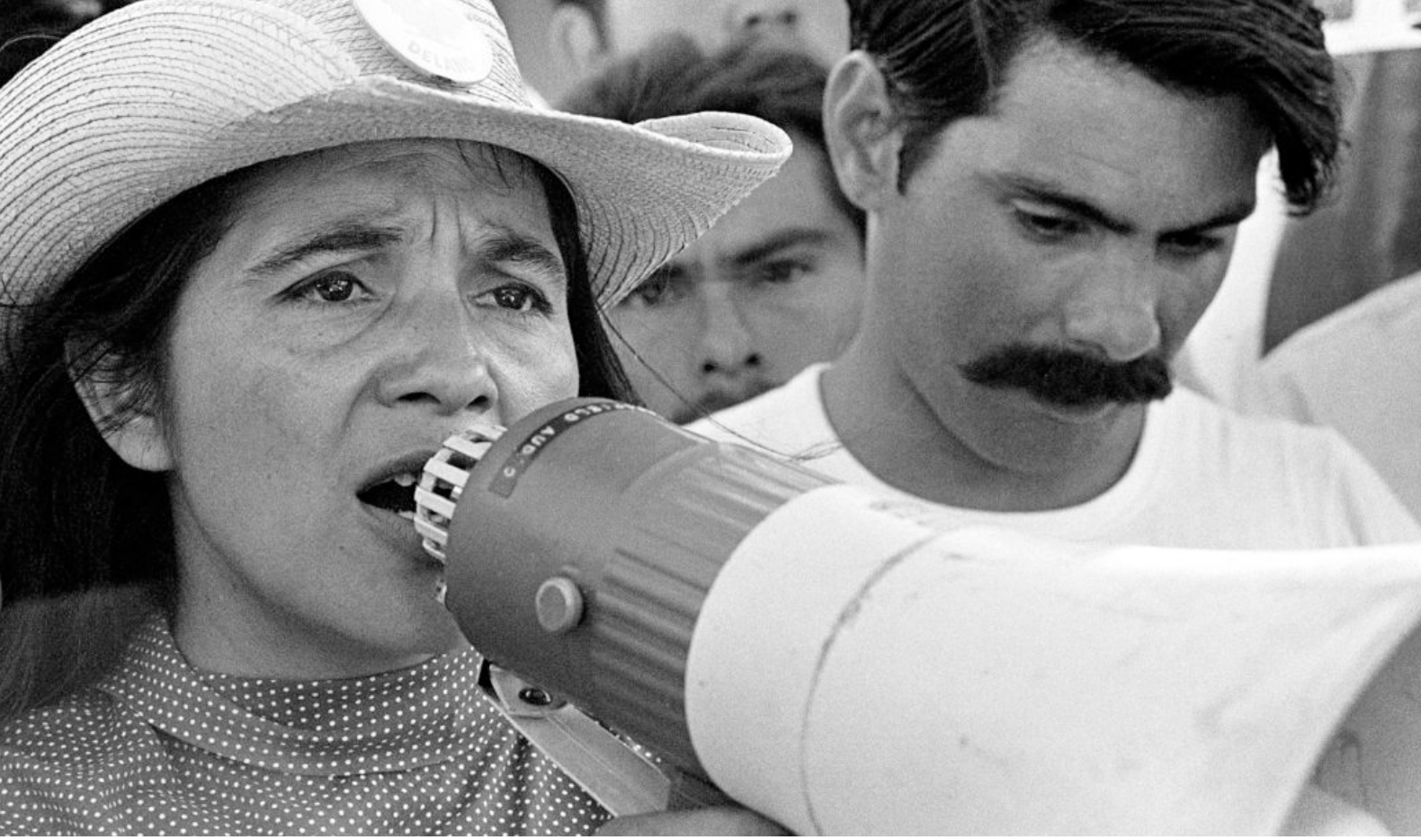
Last Wednesday, a major New York Times investigation exposed damning sexual abuse allegations against the late Cesar Chavez: an emblem of Chicano farm workers’ liberation in the 1960s. For decades, Chavez’s activism sang loudly from textbook pages, from large-scale murals and street signs across the country. Every March, his legacy was doubly hailed. He was woven into the American fabric of resistance, one championed by Black and brown workers and advocates.
Then, the testimonies arrived. Two major witnesses, Ana Murguia and Debra Rojas, explained to the Times that they were 13 and 12, respectively, when Chavez began to sexually abuse them from around 1972 to 1977. “I wanted to die,” Murguia told the Times, who confessed that she had tried to end her life multiple times as a result of her trauma from the continued abuse.
The Times investigation also included the shocking account of beloved labor leader, Dolores Huerta, who co-founded the National Farm Workers Association alongside Chavez and fellow activist Gilder Padilla. The piece touched upon two instances of coercive manipulation and rape, both of which led to pregnancies Huerta bore in secret — children that she later arranged to be raised by other families.
“I had experienced abuse and sexual violence before, and I convinced myself these were incidents that I had to endure alone and in secret,” part of Huerta’s own statement reads, which provides more context about her testimony to the Times. Huerta turns 96 on April 10th and held onto these secrets for 60 years. “I believed that exposing the truth would have hurt the farmworker movement I have spent my entire life fighting for,” she wrote.
Online, people denounced Chavez and demanded that his name and face be removed from statues and signs that decorated their local parks and libraries. These were painful, pervasive reminders of his now-soiled imprint. Local leaders promised their swift action in following through on this outcry, with Los Angeles Mayor Karen Bass signing a countywide proclamation that renamed Chavez’s national holiday “Farmworkers Day.”
Queer advocates have issued statements in solidarity with Huerta and the other survivors. In a social media post published by the San Diego LGBT Community Center, staff wrote about the ripples of fear and shame that take hold of marginalized community members when they try to reclaim their power — especially when the people they are holding accountable for abuse and harm come from notable changemakers in their own communities.
These calls for accountability do not diminish the efforts of the broader movements. “They remind us that movements are never built by one person alone,” the community center’s statement reads. “The farmworkers labor movement was built by countless individuals, many of them women and undocumented immigrants, whose organizing and resilience form its true foundation…Holding leaders accountable is how we protect every worker and every vulnerable person who the movement was always meant to serve.”
Harm can be perpetuated systemically, by forces like imperialism, as well as by the powerful within our own fights for freedom and empowerment. What holds true is that our movements do not rest solely on the efforts of one glorified leader — they are made possible by the persistent efforts of many. The farmworkers movement was brought to fruition and amplified by women like Huerta, as well as the efforts of Filipino organizers like Larry Itliong, who championed the defining Delano grape strike that uplifted and encouraged fellow farmworkers like Chavez to join in on.
Behind one venerated voice are the understated stories of several others. And what rests at this core is what the Center calls an “impossible” choice survivors of abuse face when “justice and community survival collide.” Movements for liberation are always at threat of destabilization by greater government forces: any crack in the foundation can be utilized as a dismissal of the movement as a whole. But against these narratives of fear and disempowerment, it becomes clearer and clearer that we can hold multiple truths at once.
We must believe victims who speak of their abuse: the reckoning we collectively take part in afterward cannot come at their expense or ability to heal and survive. What comes from this investigation and greater social reckoning is not the destruction of the labor movement, but of the carefully conceived and heroic portrait we’ve come to paint of Chavez’s visage within. His contributions to workers’ and farmers’ rights are irrefutable — and so is his harm.
If we discourage survivors from telling their truths in order to make precious our most visible voices, we defeat one of the pillars of why we fight at all: to strengthen our individual and combined ability to shape autonomous and shared futures that guarantee equity, freedom, and justice for every person.
Kristie Song is a California Local News Fellow placed with the Los Angeles Blade. The California Local News Fellowship is a state-funded initiative to support and strengthen local news reporting. Learn more about it at fellowships.journalism.berkeley.edu/cafellows.
Commentary
Where are our leaders? Remembering David Mixner
Karen Ocamb’s latest commentary raises a question everyone’s thinking but no one’s asking out loud: WHERE are our leaders?
I can see it with my mind’s eye. March 11. David Mixner clicks on the New York Times site and sees the headline: “U.S. at Fault in Strike on School in Iran, Preliminary Inquiry Says.” America initiated an unexplained, unprovoked, undeclared war on Iran that killed at least 168 children and 14 teachers with a deadly Tomahawk missile on Feb. 28, the first day of what has become an expanded holy war in the Middle East. Terrorist attacks on the homeland are an increasing possibility.
Mixner – a patriot and a Gandhi-influenced pacifist – is furious to the point of tears. He calls some friends, fraught with the need to “do something.” His friends agree – then one asks: “But what should we do? It’s terrible – but it’s not gay.”
“But it’s human!” Mixner roars back. “When did we lose our humanity?”
This didn’t happen, of course. March 11 is the second anniversary of David Mixner’s death, and I’m so infuriated by the deafening lack of leadership, I imagine Mixner pulling a loud alarm to roust LGBTQ+ people into action.
Where are our leaders? We’ve long known that LGBTQ+ people are at the top of the Project 2025 hit list for erasure. “The path back to national unity is to decisively win the culture wars,” Republican candidate Donald Trump told the Heritage Foundation.
We know that White Supremacists and Christian nationalists hate us. “SPLC reports that in 2024, the number of anti-LGBTQ+ groups increased by about 13% from the previous year. These hate groups “opportunistically exploit division to advance a political agenda and, in this case, it’s still informed by that false notion of LGBTQ people being dangerous to society,” says R. G. Craven, senior research analyst with the Southern Poverty Law Center.
Wayne Besen, Founder and Executive Director of Truth Wins Out, produced Behind the Mask: The Project 2025 Organizations Reshaping America, Volume I, to expose the 114 organizations listed on Project 2025’s Advisory Board. These people are dedicated to creating an authoritarian theocracy that will outlast Trump and the Iran War.
Why isn’t the Human Rights Campaign campaigning against this every day? LGBTQ+ people are hungry to “do something.” Why aren’t HRC, the Task Force, Equality Federation, and state organizations holding emergency meetings with community input to figure something out? During the AIDS crisis, Torie Osborn organized Leadership Summits that brought leaders together to strategize – many of whom also attended grassroots Creating Change events – until the Israeli-Palestinian conflict scared people away.
Where’s GLAAD? If they’re exposing misinformation, I’m not aware of it. They could revive local chapters, deputize LGBTQ+ people to be media watchdogs and do Zoom forums. They could create a free central online LGBTQ+ newsroom like Towleroad with links to reliable national, state and local news, podcasts, and Substacks so we can find out what the hell is going on.
There are 13 out members of the 119th Congress, which I learned through Google. Californians know Rep. Robert Garcia because he rose through local politics. Now he’s on TV pressing for accountability in the Trump-Jeffrey Epstein scandal. In his opposition to DHS and ICE, he sometimes mentions that he’s a gay immigrant. Rep. Angie Craig was out and pissed off after an ICE agent killed lesbian mother Renee Good, 37, who was protesting ICE’s deportation of her Minneapolis neighbors. And trans Rep. Sarah McBride has been gracefully representing her constituents and the hopes of trans people everywhere while fending off attacks from within the Chamber.
Why doesn’t the Congressional Equality Caucus hold regular Zoom town halls to give us updates, answer questions, and test out messaging with We the LGBTQ+ People?

And while we’re proudly protesting Trump, ICE, and the Iran War through Indivisible and No Kings (here’s the link to the No Kings march in LA on March 28) – remember our state and local primary races are heating up – so watch for folks who ARE showing up as leaders.
Such as Cleve Jones, founder of the Names Project AIDS Memorial Quilt, who advocated online for gay ICE deportation victim, Venezuelan asylum seeker Andry Romero. Now Cleve is working on an important new endeavor, reasserting that “healthcare is a right” as a midterm election issue. (See his Facebook page for more.)

That’s the thing about leadership. You don’t have to be rich or famous or a graduate from some elite school. Get inspired by something that grabs your heart and compels you to “do something.” Then share with others, organize, test things out to see what works and what doesn’t – and don’t give up. Remember your purpose.
And remember that leaders emerged in the post-World War II era when homosexuality was considered sick, perverted, and illegal.

Harry Hay imagined the Mattachine Society in 1948 and founded it in 1950 during the Lavender Scare period when Sen. Joseph McCarthy orchestrated witch hunts leading the House Un-American Activities Committee.
“It was obvious McCarthy was setting up the pattern for a new scapegoat, and it was going to be us – gays. We had to organize, we had to move, we had to get started,” Harry Hay told Jonathan Ned Katz for his book Gay American History: Lesbians and Gay Men in the U.S.A. (1976).
It was a crime to be gay in America, but Harry and others acted anyway. Where are our leaders now?
We don’t need perfect people. David Mixner was far from perfect. But he learned to draw from personal experience to tell and connect our real-life stories to social, political, and economic issues.
Mixner grew up shamefully closeted in rural Salem County, southern New Jersey – known as “little Dixie,” Mixner wrote in his memoir Stranger Among Friends. Segregation “was a given,” and when a “queer” died by suicide, his parents felt sorry for the teen’s parents, who had to bear that shame.
When Mixner heard Rev. Martin Luther King Jr’s call to fight injustice and watched on TV as firehoses and dogs were turned on young people in Birmingham, Alabama, the high school junior declared he was going to join their fight for freedom. Mixner and his father fought; his father hit him repeatedly and told him to “get that bullshit out of your head.”
But Mixner was a believer. When King “railed against injustice, I knew he understood the pain of being different. By working for the liberation of blacks, I intuitively knew I was fighting for my own liberation.”
Mixner had another epiphany in 1966. After reading a news story about Tempe’s garbage workers striking for the right to form a union, the buzzcut Arizona college student joined the picket line. Hector, a 50-year-old worker with a worn face and Zapata-like mustache, asked him, “Why are you here?” Mixner said he wanted to show support.
“What do you know about us? About my life – what it is like to live as we do, about fears for my family,” Hector said.
Hector’s story about his life stunned Mixner, who promised to help. It became “the first organizing project I would be responsible for from start to finish.”
The on-campus rally was small until several dozen menacing police showed up. Suddenly, students poured out of class to join the protest. Bullhorn in hand, Mixner dropped his notes and spoke from the heart about the poverty, fear, and injustice Hector and his hungry children faced every day.
“Bolstered by the crowd, I felt of value and needed,” Mixner wrote in his memoir. “The students discovered there was a whole world they had never even noticed before, and the workers found out that others cared about their plight.” Eventually, the workers got their union.
Mixner went on to become a leader in the anti-Vietnam War movement (where he met Bill Clinton), a respected political strategist, and a leader in the LGBTQ+ and AIDS movements.
He learned that political and electoral representation matters. After running LA Mayor Tom Bradley’s successful 1977 reelection campaign, Mixner came out and joined the new Municipal Elections Committee of Los Angeles (MECLA), a political action committee of political professionals and checkbook activists focused on gay rights (1977-1991).
Political relationships opened up in 1975 when the Consenting Adults Act decriminalized homosexuality in California. The bill was championed by San Francisco allies George Moscone and Willie Brown and signed into law by Gov. Jerry Brown, who was close with mega MECLA fundraiser Sheldon Adelson.
MECLA secured passage LA’s city ordinance banning discrimination based on sexual orientation. But the Religious Right turned political in 1977 and in 1978, Mixner led the fight – with San Francisco stars like Harvey Milk – to defeat Proposition 6, California’s version of anti-gay Anita Bryant’s “Save Our Children” campaign.
In 1986, extremist Lyndon LaRouche put Proposition 64 on the ballot – an Initiative that would have quarantined people with AIDS in concentration camps. Everyone did what they could to fight back. On the Eastside, AIDS activists Michael Weinstein and Chris Brownly worked with nurses and doctors to form the Stop AIDS Quarantine Committee – producing rallies and PSAs.
On the Westside, Mixner served as campaign consultant for a statewide coalition fiercely paddling upstream. The lesson from Prop 6 was the need for both volunteer-driven, grassroots mobilization and paid professional campaigners. So “Stop LaRouche” worked alongside “No on 64.”

“We were tightly coordinated,” says “No on 64” SoCal Campaign Coordinator Torie Osborn. “ AIDS phobia was so widespread that at the start of the campaign, no mainstream liberal groups – except the docs and nurses — were with us, except the Southern California ACLU chapter, and a few random Hollywood straight types, like Paul Newman. But we mobilized like crazy.”
In four months, their bi-partisan campaign raised over $2 million – 90% from the LGBTQ+ community. They defeated Prop 64 with 71% of the vote.

In the early 1990s, MECLA morphed into ANGLE (Access Now for Gay & Lesbian Equality) to focus on LGBTQ+ representation, as well as political action. In 1991, Mixner, Scott Hitt and others founded the Gay & Lesbian Victory Fund to support vetted out LGBTQ+ candidates. After Clinton won in 1992, Mixner launched the Political Appointments Program to nominate LGBTQ candidates for the Clinton administration. Clinton also lifted the ban on security clearances for gay officials.

“David Mixner loved the promise of our country, and he pushed those in power to do what is morally right. Thanks in large part to my friend David’s political prowess and strategic focus I became our nation’s first open LGBTQ+ presidential appointee to win confirmation by the U.S. Senate,” says Roberta Achtenberg, former Assistant Secretary of Housing and Urban Development (1993-1995).
Mixner encountered resistance when he advocated for lifting the ban on gays and lesbians serving in the military. But remember the humanity: the military is the nation’s largest employer, offering poor, rural gays an opportunity to get out of abuse and poverty.

Mixner felt deeply betrayed when Clinton issued the discriminatory Don’t Ask, Don’t Tell (DADT) policy. After all, Mixner and ANGLE raised $3.1 million gay dollars and supported Clinton when scandals left the presidential candidate on political life support. When Mixner protested DADT at the White House gate, Democrats made his clients disappear.

But Mixner kept networking – giving attorney and Vietnam-era Marine Capt. Tom Carpenter’s name to attorney and Servicemembers Legal Defense Network co-director Michelle Benecke. Carpenter got so involved that he became SLDN’s board chair.
David Mixner lost to Covid issues two years ago. But his legacy of leadership lives on.
“David was our national leader,” says Torie Osborn. “Mixner was a great thinker and orator — our MLK Jr. He cared about women’s and other progressive issues. I always relied on him to connect the dots and to be the ‘big picture’ guy…and inevitably he was!”
Mixner’s friend and mentee Jeremy Bernard, who became the first gay Social Secretary in President Obama’s White House, says Mixner was shocked by “how so many in his own community reacted with anger or as if he was being disloyal” over DADT. “
“This was something he really had not foreseen,” says Jeremy. David’s substantial consulting business was virtually ruined due to the White House reaction, specifically Rahm Emmanuel. One client told Mixner that they simply could not ignore Rahm’s wrath.
Mixner would struggle for years to make a living. Stranger Among Friends helped pay the bills. “But he never regretted speaking out, and time would prove him to be on the right side of history. However, few of those that loudly and harshly criticized him would ever admit that or give him any credit.”
“In 1989, David was the moving force to create ANGLE,” says attorney, politico, and longtime gay/AIDS activist John Duran. “We had suffered the deaths of tens of thousands of our people to AIDS under Reagan/Bush neglect….We elected a new President. An AIDS commission was created, chaired by ANGLE member the late Dr. Scott Hitt, and protease inhibitors were on the market three years later. Yes, ACT UP protests in the streets were essential. But there was monumental work being done with money, politics, and power.”

Like Mixner, attorney and lesbian pioneer Diane Abbitt sees the big picture about Iran. “Mixner would have been outraged at the senseless ‘collateral damage,’ the death of Americans, the death of innocent Iranian children, parents, families, the destruction of a way of life for so many, and the loss of innocence of everyone, both directly and indirectly, effected by this senseless war,” Abbitt says. “How much must people suffer? What has happened to our humanity? Where is the moral compass that should guide all people, but especially the president of the United States?”
Devastation is upon us. Where are our leaders?
Steven Guy is working with the David Mixner Memorial Fund and the Ali Forney Center to produce a film about Mixner’s activism. To support the film, reach out to Deb Brown at the Ali Forney Center at [email protected].
Karen Ocamb’s commentary is cross-posted from her Substack LGBTQ+ Freedom Fighters.

Is Trump setting a trap for White House journalists at their big dinner?

Adoption under suspicion

Lesbian cinema, from the archives and beyond, lead this short film festival

State Department implements anti-trans bathroom policy

I’m telling the scared little girl I once was it’s okay to feel free
Lesbian cinema, from the archives and beyond, lead this short film festival

Grindr to host first-ever White House Correspondents’ Dinner party

Running loud & proud: Stephen Post brings energy, advocacy, and experience to the West Hollywood City Council race

“Conscious baddies” are creating empowering queer portals across L.A.

Beloved gay romcom “The Broken Hearts Club” screens this Saturday at WeHo Park
-
 West Hollywood2 days ago
West Hollywood2 days agoLesbian cinema, from the archives and beyond, lead this short film festival
-
 White House3 days ago
White House3 days agoGrindr to host first-ever White House Correspondents’ Dinner party
-
 Commentary5 days ago
Commentary5 days agoRunning loud & proud: Stephen Post brings energy, advocacy, and experience to the West Hollywood City Council race
-
 Events4 days ago
Events4 days ago“Conscious baddies” are creating empowering queer portals across L.A.
-
 Events4 days ago
Events4 days agoBeloved gay romcom “The Broken Hearts Club” screens this Saturday at WeHo Park
-

 National3 days ago
National3 days agoInside the lonely world of MAGA gay men
-

 Cuba3 days ago
Cuba3 days agoTrans parent charged with kidnapping, allegedly fled to Cuba with child
-

 National3 days ago
National3 days agoVictory Fund brunch draws top LGBTQ officials, 2028 hopeful Andy Beshear
-
 European Union3 days ago
European Union3 days agoTop EU court strikes down Hungary’s anti-LGBTQ+ propaganda law
-
 Giving3 days ago
Giving3 days ago$20K in 20 Days for the LA Blade