
COMMENTARY
The young and the homeless
Los Angeles LGBT Center needs your help

Imagine waking up every day without money, not knowing whether you’ll have anything to eat or a safe place to lay your head at night. That’s the reality for thousands of LGBT youth in Los Angeles who are experiencing homelessness. Recently we learned just how big the problem is.
The 2017 Greater Los Angeles Homeless Count found that there are nearly 6,000 youth experiencing homelessness in Los Angeles County on any given night. Nationally, it is estimated that 20%-40% of homeless youth identify as LGBTQ. In a study of homeless youth in Hollywood, one of the most popular destinations for them, nearly 40% identified as being LGBTQ.
These are young people who’ve frequently been rejected by their families, victimized by predators, and/or made outcasts by their communities—all simply for being who they are.
Many face threats of abuse, sexual assault, and drug addiction—and the Los Angeles LGBT Center is one of the few places they can turn to for help. Since last year, we’ve been seeing more young people at our doors, turning to our youth center for three meals a day, hot showers, and access to our clothing closet. In the past 12 months, the number of visits to our youth center has increased by double digits.
But more than meeting their basic needs, including medical care and counseling, we’re helping young people develop the skills, resources, and confidence to make it on their own through GED preparation and high school completion programs, college scholarships, an employment program, leadership development program, and whatever they need to get off the streets for good.
The parents of one member of our youth center, Kenny, told him “you’re better off killing yourself” after he refused “treatment” to “cure” him of being gay. He found out about the Center’s services online and bought a bus ticket here, hoping we could help. Fortunately, we were able to give him one of our 58 beds right away, without him having to spend a single night on the streets.
But, Kenny is one of the lucky ones.
LGBT young people hit the streets with hopes of escape and a better life. Once they spend time living on the streets, they are at risk of sexual exploitation or trafficking and are likely to turn to drugs to cope with it all. Trans youth face significant challenges in entering the workforce and finding meaningful careers, so they’re even more likely to turn to sex work. Alarmingly, it’s estimated that nearly half of trans women nationwide—particularly trans women of color—will become infected with HIV if their livelihoods aren’t improved.
Lorri L. Jean is the CEO of the Los Angeles LGBT Center. (Photo courtesy of Los Angeles LGBT Center)
For nearly five decades, the Center has been caring for homeless LGBT young people ages 24 and under, and I urge you to help us get them off the streets.
If you encounter a homeless youth, tell them about the Center’s services. Our Youth Center is located at 1220 N. Highland Ave. in Hollywood, and its doors are open 7 days a week. We can connect people with a case manager 15 minutes after stepping into our facility.
Make a donation via our website at lalgbtcenter.org. Your contribution of as little as $10 will fund a full day of meals for a young person who’s depending on us for support.
You probably didn’t know that our youth center offers education support to youth who didn’t finish high school through our on-site GED preparation programs and charter high school. If you can spare a few hours a week to tutor them, contact our Volunteer Resources department at [email protected].
Drop off gently-used professional attire. The youth have access to a clothing closet so that they can present well for job interviews. Approximately 80% of the youth in our Transitional Living Program are working, in school, or both.
By giving to the Center, your support will immediately provide youth with food and a hot shower, emergency and transitional housing, education support, and employment counseling. You can give them the better life they so desperately want and deserve.

Groundbreaking on the Anita May Rosenstein Campus. (Photo courtesy of Los Angeles LGBT Center)
In two years, we will open the transformational Anita May Rosenstein Campus in Hollywood. Spanning more than a city block along Santa Monica Boulevard, this intergenerational campus will contain up to 100 beds for homeless youth (nearly double the number we currently have), new senior and youth centers, and up to 35 units of supportive housing for young people. It will be an iconic landmark that will serve as a beacon of hope and inspiration for people around the globe.
Two years is still a long time. Together, let’s make a commitment to take care of LGBT homeless youth today.






Viewpoint
I’m a queer Iranian Jew. Why I stand with Israel during this conflict
‘Hands Off Iran’ movement is erasure, not solidarity

The sirens cut through the night, jolting me from sleep. My heart pounds as I lie in bed, listening to the explosions outside. I don’t have to run — my Airbnb bedroom is a “mamad,” a reinforced bomb shelter built into the apartment. Though the windows are sealed, I can feel the building shake with each blast. This is my reality now.
I arrived in Tel Aviv just before the escalation with a delegation of North American LGBTQ leaders. We came to stand in solidarity with Israel’s LGBTQ community, which has increasingly been isolated by the global queer movement. After the delegation’s five-day mission, I had planned to stay an extra week. But on my first night here, the war broke out.
Despite the fear and chaos, I’m proud to be here. While I’m not a permanent resident of Israel — I live in Los Angeles, home to the largest Iranian Jewish community in the U.S. — I feel like I’m exactly where I’m meant to be. I work in both Iranian and Jewish advocacy spaces, and being here during this pivotal moment is an act of presence, of witness, and of resistance.
The adrenaline of seeing Israel strike back against the IRGC gave way to the sobering realization: I am in a war zone. But I know I’m safer here than I would be in many other places — because Israel protects its people. With shelters. With missile interceptors. With warnings. With a government that values civilian life.
In Iran, people don’t have that. The regime in Iran — and I use that term deliberately, because the regime is not the people — cut off internet access to prevent civilians from receiving IDF warnings before strikes. They wanted maximum casualties. They wanted suffering. They wanted images to manipulate. The same regime that imprisons, tortures, and executes LGBTQ people. The same regime that stripped my family, and millions of others, of their home.
So, when I heard the same anti-Israel activists who have spent the past 20 months calling to “globalize the Intifada” — a clear genocidal chant — adopt the new catchphrase “Hands Off Iran,” my heart sank. This is not solidarity — it’s erasure. These people defend the very regime that forced my parents to flee, tearing our family apart.
Romanticizing the Iranian regime with protest signs and slogans isn’t just tone-deaf. It’s prioritizing aesthetics over truth, trend over substance, and optics over people. It’s especially painful when I see it coming from my LGBTQ peers.
Growing up queer in the Iranian Jewish community during the ’80s and ’90s wasn’t easy. It was LGBTQ spaces that taught me how to stand tall in my truth — how to live authentically and reject shame. But now, those same spaces often turn their backs on me because I’m a Zionist, a widely misunderstood movement which simply calls for Jewish self-determination.
The hypocrisy of the current anti-Israel rhetoric is glaring. The “Hands Off Iran” movement is misguided, providing cover for a regime that tortures its citizens. Yet these activists were nowhere to be found during critical moments like the 2022 “Woman, Life, Freedom” uprisings, when Iranian women risked their lives burning their hijabs in protest. After Mahsa Amini was murdered simply for showing a little hair, those cheering “queers for Palestine” said nothing. This silence in the face of tyranny is not progressive — it’s dangerous.
For me, this conflict is not theoretical — it’s personal. I’ve witnessed firsthand how the Iranian regime targets LGBTQ people, religious minorities, and women. In Israel, I’m free to be who I am — a queer Iranian Jew. If we fail to stand with Israel, we fail to protect the values of freedom, human rights, and dignity. Israel is more than just a country — it’s a refuge for people like me, and it must remain that way.
As I write this, a fragile ceasefire is in place. But even with the quiet, the clarity remains. Israel is more than just a nation. It’s a refuge. And it’s worth standing up for — not because it’s flawless, but because it’s real. And because without it, people like me — queer, Iranian, Jewish — would have nowhere to turn.
Matthew Nouriel is a digital producer at the Tel Aviv Institute, Community Engagement Director at JIMENA, and a queer Iranian Jewish activist. He lives in Los Angeles.
Opinions
Pride and Protests: A weekend full of division
Amid more upcoming raids and protests, we will have to learn when to act, how to react and when to find pockets of joy to celebrate in, because those moments are also acts of resistance

While many Angelenos celebrated the 55th annual L.A. Pride and mainstream news outlets like ABC7 and FOX11 news covered the celebrations, the reality for many other Angelenos involved tear gas, rubber bullets and breaking news coverage from community-led outlets like CALÓ News.
If we were to take a step back into the history of Pride, we would be angered by the amount of violence and pain that led to the protests on the dawn of June 28, 1969. The Stonewall uprising took place as a result of police raids at the now-infamous Stonewall Inn on Christopher Street in New York City. The night that has gone down in history as a canon event for queer and trans life began when police raided the Stonewall Inn and arrested multiple people. The arrests and the police brutality involved, led to an uprising that lasted a total of six days.
Marsha P. Johnson and Sylvia Rivera were credited as being the first people in that historical moment to start the movement we now know and celebrate as Pride. They were Black and brown, people who transformed our notions of fear and action, modeling the mantra that we must act in order to not live in fear. The people at the Stonewall Inn on that night in June all those years ago, and all of the queer and trans people now, have something deeply unsettling in common.
We both live in a constant state of fear and anxiety.
We live in such a major state of fear that anxiety, depression and other mental health issues — including substance abuse disorders — tend to be particularly prevalent in the LGBTQ community. According to Mass Gen, the U.S. is facing a mental health crisis, with nearly 40% of the LGBTQ population in the U.S. reported experiencing mental illness last year, a figure of around 5.8 million people.
Pride began as the very type of protest that went on this past weekend over the U.S. Immigration Customs Enforcement (ICE) raids, where people have been taken into custody, reporters shot with rubber bullets and tear-gassed, and where union president David Huerta was taken into custody and charged with alleged federal conspiracy charges.
Over the weekend, I celebrated Pride. I admittedly celebrated being queer, while my other communities experienced fear in the face of arrests, tear gas to the eyes and baton blows to the head. It was an internal battle I was not prepared for and a real battle on the streets I was not ready to experience. It made me feel weak and more than anything, I felt tired. I felt scared and I felt like I was not prepared for what was to come from these arrests and this violence.
I am a proud child of immigrants. My mother is Colombian and migrated here in the early 80s, settling down in West L.A and building a life with children, houses and her religious community.
My father migrated here in the mid-to-late 80’s from Mexico, where he and his family were hardworking farmers. He has worked at his job, without rest, for over 35 years. He rose up the ranks from line worker to general manager. He does not miss work. He follows every rule and he is never late. Both are documented, but only because of luck and the ease of getting papers back when there weren’t so many bureaucratic steps to gaining citizenship or a green card legally.
My parents and their extended family are proof of a now-distant American Dream, one in which we gain status, we become homeowners and business owners, have children and send them off to college to learn things that our parents can’t even imagine.
Though they did the best they could, my parents had other challenges and barriers to their success. So I worked hard in order to succeed for them. I did it for all of the people in my communities. I did it to raise the statistics on Latinx people, LGBTQ people and former foster youth who go on to college despite the odds and get higher education degrees.
My road to where I am now was paved with uncertainty, food insecurity, homelessness and many other factors that pushed and pulled me back. The analogy I can think of to accurately compare myself to is a catapult. I was pulled down with weights that were added on more and more, until one day I catapulted forward into the life I now have the privilege to live. Though I still struggle in many ways, it is the first time in my life that I am not in survival mode. It’s the first time in my life that I get to exist as a queer person who can enjoy life, build a friend group and establish deep connections with people. It’s also the first time I get to enjoy Pride as someone who is single and who has spent the past 18 months healing from my from my last relationship.
It was the first time in my life, as a lesbian who’s been out for over a decade, that I truly planned to enjoy Pride with my groups of friends.
While I was there this weekend, my internal battle began and I felt torn between celebrating my life and my queerness and covering the ICE raid protests happening not too far from Sunset Blvd.
What I didn’t expect was to see so many other people at Pride, completely oblivious and completely disconnected from the history of Pride, instead glorifying corporate brands and companies that have remained silent over LGBTQ issues, while others have gone as far as rolling back their Diversity, Equity and Inclusion initiatives.
If Marsha P. Johnson or Sylvia Rivera were there at that moment, they would have convinced us to merge our Pride celebration with the protests. They would have rallied us all to join forces, and in the spirit of Pride, we would have marched for our immigrant community members, fighting for their right to due process.
I’m not sure if I made the right decision or not, but the next 60 days will say a lot about every single one of us. We will have to learn when to act, how to react and when to find pockets of joy to celebrate in, because those moments are also acts of resistance.
The Trump administration vowed to strip away rights and has made it their mission to incite violence, fear and anxiety among all working class, BIPOC and LGBTQ people, so it is important, now more than ever, to unite and show up for each other, whether you’re at a Pride celebration or a protest.
The next 60 days will raise our anxiety and fear, but we must remember to also take breaks, celebrate wins, relish in community, hug your loved ones and use whatever amount of privilege that you have, to show up for the communities that are hurting the most in these moments.
Juneteenth is also coming up soon and I hope to see more of us rally around our Black brothers, sisters and siblings, to not only fight for our rights, but to continue celebrating ourselves and each other.
In the words of Marsha P. Johnson: “There is no pride for some of us, without liberation for all of us.”
California
New California trans athlete policy creating ‘co-winners’ is a crock
You didn’t misread that. Hernandez shared the podium with ‘co-winners’
A lot happened at last weekend’s high school state track and field championship meet in
Clovis, Calif. Parents of cisgender student-athletes booed the one and only transgender
girl competing. Police and security officers showed up in large numbers to keep
protestors apart and safeguard the competitors. Police made an arrest outside the
stadium after a demonstrator brandishing a transgender pride flag allegedly assaulted a
man described as a conservative activist and caused damage to his vehicle.
The trans student — 16-year-old AB Hernandez — finished a winner. But she wasn’t “the” winner.
As CBS News reported, “Hernandez took home first place medals in both high jump and
triple jump and she placed second in the long jump event. Following a rule change by
the California Interscholastic Federation, a co-winner was named in each of the three
events in which Hernandez placed.”
You didn’t misread that. Hernandez shared the podium with “co-winners.”
As the Blade reported last week, the CIF introduced a new “pilot entry process” that for
the first time, allowed judges to score trans athletes separately from cisgender
competitors, so there were three winners in every event: a cisgender male winner, a
cisgender female winner and a trans student-athlete winner.
The new policy was announced hours after President Donald Trump threatened to pull
“large scale federal funding” from the state if officials allowed trans athletes to compete
according to their gender identity.
Despite the policy change, the U.S. Department of Justice announced on social
media it was investigating State Attorney General Rob Bonta, State Superintendent of
Public Instruction Tony Thurmond, the Jurupa Unified School District, and the CIF for
potential violations of Title IX, as the Blade reported.
So what happens now? As KXTV reported, President Trump issued another threat to
pull funding on Monday in a post to his Truth Social account, not naming Hernandez but
labeling her “a biological male” and using his favorite derogatory nickname for
California’s Democratic Gov. Gavin Newsom.
“A Biological Male competed in California Girls State Finals, WINNING BIG, despite the
fact that they were warned by me not to do so. As Governor Gavin Newscum fully
understands, large scale fines will be imposed!!!”
Now, the pundits are weighing-in. Sara Pequeño wrote in USA Today how she was
encouraged to see Hernandez share the 2nd place podium with Brooke White and “put
their arms around each other.”
“They’re setting an example for how all of us should treat our trans neighbors, i.e.,
treating them like human beings, not enemies,” she wrote.
As Pequeño noted, Save Women’s Sports, an anti-trans advocacy group, could only
identify five trans students in the entire United States who were competing on girls’
teams from kindergarten through grade 12 in 2023. “That group’s entire existence is to
hate trans athletes, and they found very little to hate,” she wrote.
According to the president of the NCAA, there are fewer than 10 student-athletes
who publicly identify as transgender out of the more than 500,000 competing at the
collegiate level.
Pequeño was not alone in finding joy in the rules change that brought cisgender and
transgender girls together on a podium, each of them a “co-winner.” So did self-
proclaimed “trans advocate” Cyd Zeigler.
He’s one of the co-founders of the LGBTQ+ sports site Outsports, who in 2023
infamously came close to endorsing Florida Republican Gov. Ron DeSantis for
president, only to offer his regrets, following a backlash from readers. Zeigler penned an
op-ed Wednesday originally titled “California trans athlete policy is something everyone
can embrace.”
“Everyone?” Not this sports editor.
He called the new CIF policy “the best possible path in 2025 to trans participation in
sports.”
In celebrating this change, Zeigler also trashed “goal-post-moving trans advocates” and
policies in California and Connecticut that allow “a trans girl to run in boys track meets
and, without a medical transition, later compete in girls meets,” meaning high school
competitions. “That’s bad policy,” declared Zeigler without evidence.
That policy in Connecticut has stood since 2011 and is enshrined in state law, and so far
has withstood legal challenges once again being heard in federal court.
Outsports at some point changed the headline of his screed to “New California trans
athlete policy is something we can embrace” and apparently made another significant
choice: Despite quoting the outlet’s one and only remaining transgender contributor,
Karleigh Webb, who opposes the rules change, Zeigler did not mention her by name.
Why?
In an article published before the championship, Webb wrote: “If AB Hernandez wins,
why should she have to share the spoils with someone else if’s not a tie? That’s what
professional transphobes like Jennifer Sey and Riley Gaines try to sell. Awarding a
duplicate medal gives their nonsense credence to the detriment of the sport and the
athletes.”
Webb is right. Zeigler and the CIF and Gov. Newsom are wrong. You either win, or you
lose, or if you prefer, you come in second, third, whatever. But “co-winners?”
That’s a crock.
Imagine if the Dodgers and Yankees shared the World Series trophy. Why shouldn’t the
49ers also win the Super Bowl alongside the Chiefs? Maybe Kamala Harris should be
declared a “co-winner” of last November’s election?
Personally, I’m glad to see Hernandez embraced by her cisgender peers. I’m relieved to
know that crowds cheering these amazing girls last weekend drowned out the hecklers
who showed up to boo a child. I’m encouraged that even if she had to share the win,
Hernandez was given her rightful place among the teens competing and proved she
was not only worthy of competing but did not win in every event.
So, she’s hardly “unbeatable.” Most trans athletes actually lose, as Zeigler wrote almost
six years ago, back before he started echoing anti-trans inclusion activists Martina Navratilova, Renee Richards and Nancy Hogshead-Makar.
If he really thinks the CIF “co-winners” rule is going to silence anti-trans forces, I think
he’s going to be very surprised by Riley Gaines and her crowd.
While it’s easy for Zeigler to concede public opinion has shifted, he should know
better than to blame those who pushed for inclusion, when it’s clear that conservative
voices in media and politicians, like his, are the ones responsible for influencing that
move to reject trans women’s right to compete in women’s sports. It’s a pendulum swing
that in time will undoubtedly swing back, once the science proves that trans women and
girls don’t always win. In fact, researchers have already proven some trans athletes are
at a disadvantage compared to their cisgender competitors.
Just as Parker Molloy reported that a Republican-commissioned study on gender
affirming care in Utah actually found “that youth who received care before age 18 had
better outcomes, especially around depression, anxiety and suicidality. Hormonal
treatments were associated with positive mental health and psychosocial functioning
outcomes.”
I believe the science is on the side of transgender Americans. Americans love a
winner. Not a “co-winner.”
Opinions
Trump’s inhumanity won’t erase Andry Hernandez Romero, if we resist
Andry Hernández Romero’s case continues to be a violent reminder that we must rise up and resist
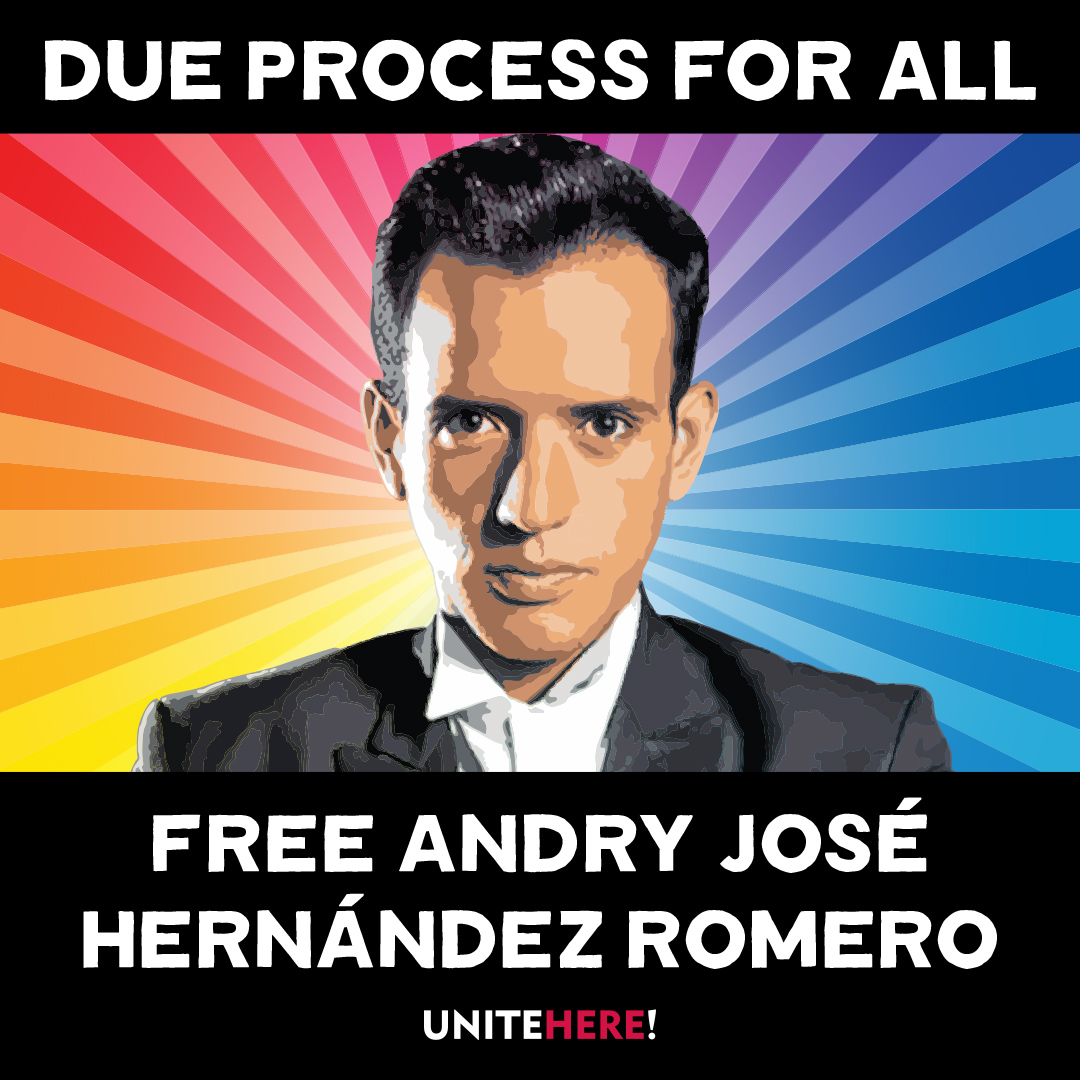
Editor’s Note: Since this article was first published, more information on Andry’s case has become available.
UPDATE: On June 4, a federal judge ruled in favor of the ACLU and Democracy Forward in J.G.G. v. Trump, in which deported gay stylist Andry José Hernández Romero is one of the lead plaintiffs. Describing the Venezuelan deportees’ situation as Kafkaesque, Judge James E. Boasberg said the plaintiffs would likely prevail in their complaint about being denied due process, the New York Times reported. Trump officials, Boasberg wrote in his 69-page ruling, “spirited away planeloads of people before any such challenge could be made. And now, significant evidence has come to light indicating that many of those currently entombed in CECOT have no connection to the gang and thus languish in a foreign prison on flimsy, even frivolous, accusations.”
“Absent this relief,” the judge wrote, “the government could snatch anyone off the street, turn him over to a foreign country and then effectively foreclose any corrective course of action.” He ordered the Trump administration to give the deportees the due process they have been denied.
On Friday, June 6, Rep. Pramila Jayapal (WA-07), Ranking Member of the Immigration Integrity, Security, and Enforcement Subcommittee, will host a shadow hearing Kidnapped and Disappeared: Trump’s Lawless Third Country Disappearances at which Andry’s attorney Lindsay Toczylowski will testify.
The juxtaposition is morally excruciating. The very air in West Hollywood is electric with
queer joy and the excitement of WeHo Pride, but it’s more than a celebration of our ongoing
movement for liberation and equality. We’ve been waiting for a moment to exhale and
stop the clamor of the Trump horror show.
What can we do to stop this overwhelming dictatorship campaign that is gleefully
enforcing Project 2025 through a deluge of cruel Executive Orders, demonizing and
erasing anything under Diversity, Equity and Inclusion initiatives and LGBTQ while dispatching masked ICE agents to snatch anyone Trump’s White Supremacist terrorist administration tags for deportation.
Among those swept up in Trump’s frenetic crusade is Andry Hernandez Romero, a 32-
year-old gay hair stylist and makeup artist who fled harassment and threats of violence in Venezuela in May 2024, after speaking out against authoritarian dictator Nicolás Maduro. After navigating the complex app designed to streamline the byzantine U.S. lawful entry process, last August Romero faced a U.S. border official in San Diego. With no criminal history, he demonstrated a “credible fear of persecution” to proceed with an asylum case.
Imagine what Romero felt — so close to freedom, to opportunity, to unabashed queer joy.
Then came that Trumpian twist.
During a physical exam, officials fixated on Romero tattoos of crowns with the words “Mom” and “Dad.” The agent apparently assumed that Venezuelan gangs accept gays because he suspected Andry had gang affiliations and does not fact check because Tren de Aragua does not use crown tattoos for gang identification.
Romero landed in detention awaiting his asylum court date. But one week before the
March 13 hearing in San Diego, Romero was abruptly transferred to a facility in South
Texas, resulting in his absence in court. The hearing was postponed to March 17 when
the immigration judge again asked where Romero was.
“He was removed to El Salvador….we just found out today,” the ICE lawyer replied. The judge questioned the legality of Romero’s deportation without a removal order.
On March 14, Trump invoked the Alien Enemies Act — a 1798 law used during a
declared war — to target immigrants as government “enemies” who had “infiltrated”
America. Secretly, ICE deported Romero and 137 other Venezuelans to El Salvador’s
notorious Terrorism Confinement Center, with Trump paying dictator President Nayib
Bukele to incarcerate the kidnapped immigrants.
The world watched as Andry and his shackled fellow prisoners were displayed on TV
brutally forced off the plane and forced to kneel as agents roughly shaved their heads.
TIME Magazine photographer Philip Holsinger reported that Romero was being slapped while crying out for his mother, “I’m not a gang member. I’m gay. I’m a stylist.”
Trump called the Venezuelans “rapists,” “savages,” “monsters” and “the worst of the
worst,” claiming they were thoroughly vetted. But ProPublica reviewed each case of the
Venezuelan deportees and reported that the Trump administration knew that “the vast
majority” of the 238 Venezuelan immigrants ”had not been convicted of crimes in the
United States before it labeled them as terrorists and deported them, according to U.S.
Department of Homeland Security data that has not been previously reported.”
Lee Gelernt, the American Civil Liberties Union’s lead attorney fighting the deportations,
told ProPublica that the removals amounted to a “’blatant violation of the most
fundamental due process principles” and subjected the deportees to life imprisonment.
There have been numerous attempts to look for a humanitarian bone in the Trump
administration’s body politic, most notably gay immigrant Rep. Robert Garcia’s heated
exchange with Homeland Security Secretary Kristi Noem during a May 14 congressional hearing. Garcia (D-Long Beach) went to El Salvador for a welfare check
but was denied access to Romero.
“He has had no access to lawyers or family since he has been taken over a month now,”
Garcia told Noem. “His mother just wants to know if he is alive.”
“I don’t know the specifics of this individual case. This individual is in El Salvador and
the appeal would be best made to the president and to the government of El Salvador
on this,” replied Noem.
Garcia pushed back.
“You and the president have the ability to check if Andry is alive and is
not being harmed. Would you commit to at least asking El Salvador if he is alive?”
Nope.
“This is a question that’s best asked to the president and government of El
Salvador,” she said.
Noem’s callous disregard for life and suffering is unsurprising. The former governor of
South Dakota blithely noted in her political memoir that she shot and killed her 14-
month-old dog Cricket when the puppy misbehaved. “I hated that dog,” Noem wrote.
She also shot a goat she didn’t like.
“In neither case did Noem show any doubt or remorse; quite the contrary, she sought to
cast her action as a signifier of tough-minded realism that would burnish her appeal as a
politician from a rural community,” wrote Sara Amundson, president of the Humane
Society Legislative Fund.
So if Noem thinks callousness is cool, imagine how she feels about someone she might
deem as sensetive?
“Under the Constitution, every single person has a right to due process, and that means
they have a right to notification of any allegations the government is making against
them and a right to go into court and prove that those allegations are wrong if that’s the
case,” Lindsay Toczylowski, President of the Los Angeles-based Immigrant Defenders
Law Center who is representing Romero pro bono, told NBC News San Diego April 11.
“In Andry’s case, the government never gave us that opportunity. In fact, they didn’t even
bring him to court, and they have forcefully sent him to El Salvador without ever giving
us any notice or without telling us the way that we could appeal their decision.”
On May 27, Immigration Judge Paula Dixon granted a U.S. Dept of Homeland Security motion to dismiss asylum proceedings for Romero scheduled for the following day.
“We should all be incredibly alarmed at what has happened in Andry’s case. The idea
that the government can disappear you because of your tattoos, and never even
give you a day in court, should send a chill down the spine of every American. If this can
happen to Andry, it can happen to any one of us,” said Toczylowski.
Andry’s life depends on us holding the Trump administration accountable for what they
have done to him,” Toczylowski said. “We will continue to fight until Andry is safe and
free.”
Romero is a lead plaintiff in the American Civil Liberties Union’s and Democracy Forward’s J.G.G. v. Trump case in which Romero’s friend and mother gave statements that are now evidence saying Romero “was persecuted both for his sexual orientation and for his refusal to promote government propaganda” while working as a makeup artist at the TV network in Caracas, according to CNN.
But Project 2025 booster Kevin D. Roberts doesn’t care, having ordered the Trump
administration to delete “the terms sexual orientation and gender identity….out of every
federal rule, agency regulation, contract, grant, regulation, and piece of legislation that
exists.”
So do Trumpland judges care about the raison d’etre for asylum or is that too DEI?
NBC News reported that Romero’s dismissal order “allowed for the possibility that the
case be reopened if Hernandez returns to the U.S.”
That’s why we the people, must rise up and resist.
“As the son and grandson of Japanese Americans who were rounded up and forced into
camps without due process, I know all too well that Andry is not the first person to be
unjustly taken by the government,” says out Rep. Mark Takano (CA-39), Chair of the Congressional Equality Caucus. “Every American should be alarmed by how openly the
Trump Administration is taking people off the street and locking them away in a foreign
prison without so much as a day in court — all because of their tattoos. This fight is not
over yet, but every day it drags on puts Andry and others’ lives in danger. I stand with
Andry, his family, his lawyers, and our Constitution in rebuking President Trump’s cruel
and illegal attacks, and hope that justice is swiftly served.”
Longtime activist Cleve Jones urges all LGBTQ people and allies to take action.
“We don’t know if he’s dead or alive,” Cleve says. “I look at [Romero] and he’s like my little
gay brother who is now in this terrible situation where he — if he is still alive — is probably
being subjected to horrendous brutality on a daily basis.”
But Cleve is also angry at the lack of response to this urgently important case.
“If you want to be intersectional and not just quack about it, look at this case,” Cleve
says. “This young man stands at the intersection of our fight for LGBT equality, for
immigrant rights, and for due process under law.”
San Francisco Pride and New York City Pride rejected his request to name Andry an
honorary Grand Marshal. But, Cleve says, “I’m happy that a number of pride
celebrations have done that. Others have stepped up and are organizing fundraisers. I
see there’s one coming up in New York. But everybody should be talking about Andre.
Free Andre. Free Andre. It’s so important!”
Please note: To support Romero’s case and others like it, the Immigrant Defenders Law Center is selling a T-shirt that says “Asylum is a Human Right, found here.“
Commentary
On Pope Francis, Opus Dei and ongoing religious intolerance

“Good Friday” set the stage for Saturday’s anti-Trump/MAGA “Hands Off” protests serving as a timely lead-in to binge-watching Alex Gibney’s two-part HBO political documentary, “The Dark Money Game” on Easter Sunday. In “Wealth of the Wicked,” nefarious Opus Dei —Svengali Leonard Leo strategically seduces politically disappointed Catholic Federalist Society billionaires into subsidizing a scheme to ‘pipeline’ malleable conservative judges to take over the Supreme Court and overturn reproductive rights.
A key victory for “Operation Higher Court” came in 2010 when SCOTUS ruled 5-4 in Citizens United v Federal Election Commission, that corporations and unions have the same First Amendment free political speech rights as individuals—as long as their unlimited cash donations go to 501 c(4)’s or Super PAC slush funds and not directly to candidates. Twelve years later, in 2022, they got their payoff with the overturning of Roe v Wade by Leo-promoted Catholic justices.
But Leo’s political conniving is not the only exploitation of moral corruption. The documentary exposes conservative Christians too.
Gibney’s anti-hero is a former rabid anti-abortion lobbyist named Rev. Robert Schenck. He tells of turning to a fellow conservative in Cleveland, Ohio after Trump won the Republican presidential nomination in 2016 and asking: “Are we really going to do this? We’re going to choose this man who’s inimical to everything we believe?” The other evangelical replied: “I don’t care how bad he is. He’s going to get us the court we need.’”
Schenck explains the unholy alliance between Christian conservatives and Big Business. “Whenever you talked about government regulation, the argument was eventually —‘these same characters who control my business are going to start trying to control your church. So, it’s in your best interests that we defang this monster’— and that brought a lot of religious conservatives over.”
And there’s this: “We have a little aphorism built on a Bible verse: ‘The wealth of the wicked is laid up for the righteous.’ So, yeah, let’s baptize the billionaires’ money. We can do that — and it eventually brought together this alliance.”
Schenck later reveals an intense epiphany that resulted in regret for how much harm he caused. Not so for Leo.
This is an excerpt from Gareth Gore’s comprehensive book Opus, for Rolling Stone Magazine:
“DURING THE DONALD TRUMP YEARS, conservatives — led by Leonard Leo — took control of the Supreme Court…. At one Federalist Society event, his good friend Supreme Court Justice Clarence Thomas jokingly referred to Leo as the third most powerful man in the world, presumably behind the pope and the president of the United States.”
On Monday morning, Pope Francis died. I liked this pope, compared to the others. I covered Creating Change during the AIDS crisis when author Paul Monette delivered his brilliant, scathing denouncement of the Catholic Church, then unexpectedly ripped up a portrait of Pope John Paul II. Pope Benedict XVI was just crotchety cruel. But Pope Francis —named for St. Francis of Assisi —had that big smile and genuinely seemed to care about migrants, the vulnerable and the marginalized — like us. He even used the word ‘gay’ instead of ‘homosexual.’
Pope Francis’ reply to a question about a Vatican “gay lobby” on a flight from Rio de Janeiro to Rome made global news. “If a person is gay and seeks God and has good will,” he said in 2013. “Who am I to judge? We shouldn’t marginalize people for this. They must be integrated into society.”
What did this mean? Welcoming inclusion into a family that officially considers us ‘intrinsically disordered?’
And then there was Pope Francis’ interaction with Juan Carlos Cruz — a whistleblower in Chile’s clerical sex abuse scandal.
“He said, ‘Look Juan Carlos, the pope loves you this way. God made you like this and he loves you,'” Cruz told The Associated Press.
Meanwhile the Catholic Church Catechism affirmed, “this inclination, which is objectively disordered, constitutes for most of them a trial.”
Ergo, a behavioral choice.
Therein lies the problem.
LGBTQ people are seen largely as individuals with sinful same sex sexual ‘inclinations.’ So when the pontiff touted ‘the equal dignity of every human being,’ and rebuked Vice President JD Vance with the ‘Good Samaritan’ parable, whereby love “builds a fraternity open to all, without exception” — we are still the exception.
Francis was all also human — having to apologize at one point for using a gay slur. But what of the bigger things like, did he know about the Opus Dei takeover of the U.S. Supreme Court when he chastised Vance about deporting migrants? Did he know that the Archdiocese of Los Angeles agreed to pay $880 million to 1,353 people last October, who allege they were victims of clergy sexual abuse? With a previous payment of $740 million, the total settlement payout will be more than $1.5 billion dollars. Is Leo chipping in to replenish that?
And it’s not over. Earlier this month, Downey Catholic priest Jaime Arriaga, 41, was charged with several counts of child sexual abuse which allegedly happened when he was serving as a transitional deacon at the Our Lady of Perpetual Help Church.
Longtime U.K LGBTQ+ activist Peter Tatchell — who’s campaigned against Catholic homophobia for 58 years — says Pope Francis’ legacy is complicated.
“I extend my condolences to Catholics worldwide on the passing of Pope Francis. While we often disagreed on issues of LGBTQ rights, I acknowledge his more compassionate tone towards sexual minorities. His recent moves to allow blessings for same-sex couples, albeit with limitations, signaled a small but significant shift in Church doctrine,” Tatchell said in a statement.
“However, for millions of LGBT+ people globally, the Catholic Church remains a force for discrimination and suffering. Under his leadership, the Vatican continued to oppose same-sex marriage and trans rights. Catholic bishops lobbied against the decriminalization of homosexuality in many parts of the world. The Vatican still upholds the homophobic edicts of the Catechism, which denounces the sexual expression of same-sex love as a ‘grave depravity’ and ‘intrinsically disordered.’ Francis’s legacy is, therefore, a mixed one — offering some progress, but leaving deep-rooted inequalities largely intact.
“The struggle for LGBT+ equality against a homophobic Church must continue. We urge the next Pope to go further—to end the Church’s support for discrimination, both within the faith and in the wider society.”
Opinions
Gay for pay: Andy Lee and the changing face of content creation
Are the lines between identity and performance more fluid than we’re ready to admit?
In today’s ever-fapping world, the intersection of sexual identity and content creation has become more complicated than ever. Irish content creator Andy Lee, cozily ranking in the top 0% of OnlyFans creators, with his furry physique and tatted up torso, is at the center of the conversation. A self-identifying hetero who rose to prominence during the Pandemic, Lee has amassed a girthy following of horny gays, likely because of the exclusive man-on-man content he has to offer. Yet, his success raises just as many eyebrows as it does trousers. Many question the authenticity of his content, sexual identity and whether or not straight men are overshadowing their openly gay peers.
Claiming to be straight only to then go pole-to-pole on camera, Lee is seen by a significant portion of the queer community to be guilty of queerbaiting (exploiting gay culture for profit). Others can’t help but wonder, is this slab of man-meat genuinely drawn to the physical (and perhaps emotional) experiences he has with men, despite identifying as a thorough(ly) bred breeder?
Lee’s OnlyFans career showcases the blurred, often contradictory nature of sexual identity. He enjoys sexual experiences with men but still identifies as straight, which challenges traditional labels like “gay” and “straight.” His content forces us to confront the nuanced lines of sexual identity, which are rarely ever clear-cut and often defy simple categorization.
The question of authenticity also hangs in the amyl nitrite-scented air. While Lee has said his career on OnlyFans has made him feel “wanted and loved” (and paid) by the gay community, many argue that his identity as a straight man undermines the emotional connection his audience thirsts for. Is his content less authentic due to its “no-homo” viewer discretion warning, or does his openness to explore other men’s bodies reflect the evolving, fluid nature of human sexuality?
This has led to several openly gay performers to claim that, well, “they’re taking our jobs.” They argue that by creating gay content for profit, straight men commodify gay experiences while avoiding the brunt of the stigma that accompanies being openly gay. But how valid is this criticism? In a consumer-driven adult content market, if people choose to engage with Lee’s content, are they unintentionally depriving the gay sex-working community?
And then there is the aspect of the gay gaze (did not stutter). Is it the allure of the forbidden nature of straight men giving into the carnal pleasures that another man has to offer? The taboo? The challenge? Or are they simply the proxy of the coach you had a crush on in high school, the hot trainer who you overheard has a girlfriend, or that college professor you once stood next to at the urinals only to find out for yourself just how extensive his curriculum was? For many, this particular brand of tension is a huge part of the turn-on.
This paradox is just one part of a broader cultural conversation about masculinity and sexual identity. Straight men in gay content can subvert traditional gender roles, while simultaneously reinforcing certain ideals of masculinity. In cases like Lee’s, when a straight man openly enjoys the physical pleasure of being with other men, it speaks to both the complexity and fluidity of sexual identity, and the inability of inflexible labels to accurately and respectfully encompass human desire.
Ultimately, the conversation around gay-for-pay creators like Andy Lee isn’t black and white, straight or gay. Although likely unintentional (let’s be real), these performers challenge existing ideas of identity, authenticity, and the commodification of desire. Whether Lee is queerbaiting, exploring his own sexuality, or just making stacks of cash, his presence in the adult content world invites folks to rethink how we define sexual identity today. Just something to think about next time you’re… enjoying content.
AJ Sloan is a writer, retired adult performer and clinical counseling graduate student. His work has been featured in Huffington Post and The Advocate and led his own weekly column for Fleshbot.
Opinions
Why is it important for cities to become LGBTQ sanctuary cities?
This is not just a win, it is a small, but monumental stride toward progress, representation and protection

When a city passes the motion to make their city an LGBTQ sanctuary city, it means that city or state resources cannot be used to prosecute or punish LGBTQ people for seeking gender-affirming care, resources or government assistance.
As many of us know, there are three major levels of government: local, state and federal.
City motions set a precedent for the state, adding local representation on a small scale that hypothetically catches on and makes its way up the ladder to the state, then federal level.
Though the Trump administration holds a lot of power on a federal level, states, cities and municipalities hold power on a level that is easier for local communities to change and control. If cities across the state begin passing motions to become LGBTQ sanctuary cities, the state then has to consider passing the motion to become a sanctuary state. If the majority of states consider themselves sanctuary states, it pushes the change on a national, or federal, level.
At first glance, it seems like the move for a city to consider itself an LGBTQ sanctuary city is not a big deal because there is no financial flow in the motion and there are no special funds to be allocated. The only visible change is the new title the city gets to claim. However, passing motions in favor of LGBTQ rights, is crucial toward the longer and harder journey to attain rights on a national level. It is a far more nuanced issue than what it seems.
If that same logic were to hold up when it comes to statewide decisions, then it could become easy to dismantle progress made on any level.
The Advocate published an article in November when the City of Los Angeles unanimously passed the ordinance to become an LGBTQ sanctuary city. Passing the ordinance means that the city is now responsible for “shielding queer youth who travel to the city to receive gender-affirming care from prosecution, as well as preventing city resources from being used in immigration enforcement or assisting federal immigration officials.”
During the November 2024 election, Proposition 3 made it on the ballot and Californians had the choice of voting in favor or against the proposition that would only change the outdated language of the California state constitution, that until recently did not recognize same-sex or interracial marriages. To some, the change seemed meaningless, but on a statewide level, passing this proposition meant cementing the progress made on the protection of same-sex and interracial marriages. Though the proposition had no money flow in the matter, this important move signaled the support of the state in favor of LGBTQ rights on a state level.
While California is already a sanctuary state, it is also crucial to recognize protections and rights in individual cities. During these unprecedented and uncertain times in LGBTQ history, it is more crucial than ever to push for these changes.
When one city makes the move to become a sanctuary city, others follow and LGBTQ representation becomes more visible on a government level.
In November, shortly after Trump was elected as the 47th president of the United States, Los Angeles declared itself an LGBTQ sanctuary city.
Now, Long Beach has followed suit and has unanimously approved a resolution to make the city a transgender sanctuary city and officially recognize March 31 as Trans Day of Visibility.
There are a growing number of LGBTQ sanctuary cities across the nation. In California, the list of cities includes San Francisco, Sacramento, West Hollywood, Los Angeles and most recently, Long Beach.
Other cities, including Boston, Massachusetts; Olympia, Washington; Cambridge, Massachusetts and others across the nation have also recently declared their status in support of LGBTQ people.
This is not just a win – it is a small, but monumental stride toward progress, representation and protection. We need more cities to push motions to become sanctuaries for queer and transgender people as the current administration continues to use queer and trans people as political pawns in the chess game rigged for the alt-right.
Miscellaneous
Gay bar in California bans MAGA gear — but no other political expression — from its premises
MAGA is a terrorist threat to the LGBTQIA+ community
Do not let anyone bait you into a “both sides” argument on this topic. Trans people can confirm that we no longer live in a country where freedom of expression exists in the first place, so the point in and of itself is moot. Don’t waste your energy.
But especially don’t be shamed by those who imagine themselves to be more enlightened than you as they make the tired false equivalence that MAGA is just another political ideology that deserves the same freedom of expression as liberal points of view.
The owners of the Badlands Bar are keeping their patrons safe from terrorism. Yes, MAGA is a terrorist threat to the LGBTQ community. Oxford’s definition of terrorism is “the unlawful use of violence and intimidation, especially against civilians, in the pursuit of political aims.”
It’s too long a list for this article, so here’s a link to a running tally of the government’s actions against the LGBTQ community since Jan. 20.
It started, on Trump’s first day as president, with trans people being forcibly stripped of their very identity — and with it, all protections — under the law. This trend has continued, ominous drip after ominous drip of frequently illegal Executive Orders that dehumanize, disenfranchise and dismantle the basic rights and dignities of trans and queer Americans. If you’re following the Project 2025 playbook, as the federal government is, you’ll notice that ending marriage equality is quickly coming up on MAGAs To Do list.
All of that—the bullying, the emotional and psychological abuse, the stripping of rights, the (eventual, inevitable) tearing apart of families—is violence, by definition. The anxiety you feel every day as an LGBTQ American? That’s intimidation. And that is why living under MAGA as an LGBTQ person means living in a terrorist state.
Perhaps the idea that MAGA perpetrates outright terrorism seems dramatic, especially for those who remember 9/11 and maybe we don’t need to add more drama to this historical moment.
Then let’s consider the terrorism of words and ideas.
Stochastic terrorism, is a particularly nasty form of political expression, where those with cultural power spout hostile rhetoric about a group, creating a culture of hate that inevitably — but not directly — results in violence. When we talk about haters becoming emboldened by Trump’s rhetoric, this is the dangerous potential that absolutely does become reality.
The insidious part of stochastic terrorism is that there’s plausible deniability on the part of the instigators. Truly, who do we blame for the murder of Lauri Carleton in Lake Arrowhead, CA?
Do we blame the individual who shot her after he screamed epithets about the Pride flag she flew in front of her store? Or do we blame the talking heads and podcast hosts who were then spending untold airtime equating LGBTQ people with pedophilia and grooming? Or do we blame the governors who sought to ban the flying of Pride flags in public, for turning them — and all of us who fly them — into high-profile lightning rods for hate? Who should be charged in a court of law for this hateful crime?
If any comparison to terrorism still seems too far-fetched to you, even for MAGA, then let’s consider the term “gang.”
Flip all the racist rhetoric you’ve passively absorbed about the kinds of people most likely to be in a gang, and consider Donald Trump, the current Republican Party, and MAGAs specifically as you read the following definitions of what a gang is.
According to the Department of Justice:
- Gangs adopt a group identity in order to create an atmosphere of fear or intimidation.
- Gangs are typically organized upon racial, ethnic, or political lines and employ common names, slogans, symbols, hand signs, or style of clothing.
- The gang’s primary purpose is to engage in the use of violence or intimidation to enhance or preserve its power, reputation, or economic resources.
If we hold MAGA to the DOJ’s gang standards it so easily fits into, perhaps we can more easily hold that most businesses explicitly bar gang symbols from their premises, often as an easily-enforcible safety measure, and consider the Badlands Bar owners’ actions in that context.
But if you’re still suspicious of any of this rhetoric, then all that’s left is to consider the reality of MAGAs actions, which owners of LGBTQ bars around the country experience on a regular basis.
On Feb. 22 at Scorpio, in Charlotte, NC: an exception made to a “no political affiliations of any kind” dress code, devolved into the individual making transphobic remarks at the entertainers during the drag show. He refused to leave when asked and became aggressive toward security, resulting in police intervention.
On March 14 at the Chatterbox Jazz Lounge in Indiana, MAGA hat-wearing patrons aggressively misgendered and harassed a bartender and were ejected. The video of the altercation went viral; the owner reports his bar has since received several threats of arson and bodily harm.
Four days after the video of that incident went viral, the Chatterbox Tavern in Tennessee received threatening emails and phone calls.
These incidents were flashpoints that reported, often by MAGAs claiming victimhood. Untold incidents go unreported due to intimidation or uninvestigated due to bias. According to GLAAD’s 2022-24 ALERT Desk Report, over 1,850 anti-LGBTQ incidents were reported across all 50 U.S. states. That’s more than 600 acts of vandalism, bomb and mass shooting threats, assaults, and cases of arson per year — nearly two per day. These incidents have resulted in at least 161 injuries and 21 deaths. The perpetrators — when apprehended or known — wore MAGA gear, screamed MAGA slogans, had shared MAGA rhetoric online, or were members of MAGA-associated groups like the Proud Boys, Q-Anon, Three Percenters, Libs of TikTok and Moms for Liberty.
If after all of this — and the rest yet to come — you still believe that MAGA simply represents an opinion about a stance on taxes, individual liberties and the size of government, then this author will be the bigger person and acknowledge your identity as part of America’s inherent Diversity, wholeheartedly Include you as an Equal in this vast multiplicity to which we belong called America.
And then ask you, if it’s all directly equivalent: when will MAGA do the same for LGBTQ people?
Of course you are free to wear your red hat and shirt wherever you please — your gang runs this place, after all. You’ll even be pardoned for violence you commit, like the Jan. 6 terrorists and your poster boy Kyle Rittenhouse. Don’t fret.
But don’t expect us not to protect our own just because we’re a bunch of queers.
The author of this Op-Ed wishes to remain anonymous for safety reasons, given the nature of the issues discussed. Citations are linked to GLAAD’s expert resources, but this Op-Ed was not written by anyone affiliated with the organization.
Opinions
Newsom is playing right into the far-right’s playbook
A democratic political leader who built a reputation on standing ten toes down for the LGBTQ+ community and being the political rebel that Trump has vowed to take down, has seemingly joined the dark side.
Late last month, California Governor Gavin Newsom released the first episode of his new podcast titled, “This is Gavin Newsom.” This week, he released the second episode featuring his first guest, Charlie Kirk.
Kirk is a 31-year old conservative “activist” and founder of the right-wing student organization Turning Point USA. The episode gained media attention because Governor Newsom has always stood behind LGBTQ+ rights and has always been a vocal advocate for LGBTQ+ protections on the local, state and federal level. He has gained political support and built an entire career on the backs of LGBTQ+ Californians and what he seems to be forgetting right now, is that LGBTQ+ includes the transgender community.
The trans community is one of the most politically vulnerable communities who are constantly undergoing heavy, hateful and misinformed political attacks.
It came as a shock to hear Gov. Newsom speak on this issue and sound just like a far-right republican who’s been against trans Americans since the very beginning. During his two terms, he has advanced LGBTQ+ protections and fundamental rights by signing laws that cement rights.
In contrast to all this progress he’s advocated for, he took the stance against allowing trans athletes to participate in women’s sports – a hard betrayal to the community that was counting on him more than ever. The current administration is hostile and extreme in their attempts to erase gender nonconforming and trans people and a politician like Newsom, was a diamond in the rough when it came to LGBTQ+ issues.
“I revere sports and so the issue of fairness is completely legit,” said Newsom in his podcast episode. He was referring to his view on fairness regarding trans women and young girls in women’s sports competitions.
Many organizations and leaders across California have responded to his views of trans women competing in women’s sports.
CEO and founder of TransLatin@ Coalition responded with outrage and disappointment.
“The TransLatin@ Coalition is extremely disappointed and enraged about the remarks made by Governor Gavin Newsom on his podcast on the issue of trans youth participating in sports,” said Salcedo in an Instagram post.
The Coalition called out his message about trans athletes by mentioning his need for support from conservatives for his potential bid for presidency.
“This is probably a stunt by our governor to align with conservatives to set himself up for the presidency, but he is fooling himself if he thinks this is the route.”
Around the same time, the Los Angeles LGBT Center issued a statement condemning his exclusionary message about trans athletes.
“Newsom is parroting the same Republican talking points used to marginalize and erase trans people,”said Joe Hollendoner, CEO of the LA LGBT Center. “This is an appalling betrayal from someone who once positioned himself as a champion of equality and demonstrated such strong leadership on behalf of LGBTQ+ people during the first Trump administration.”
What Newsom and the alt-right extremists who use the fairness argument in response to trans athletes need to understand, is that trans rights are not up for debate.
Athletes, trans or not, should be able to compete freely in sports under the First amendment.
If it were a matter of fairness, they would also consider it unfair to have trans men compete in the male divisions of sports, yet they are not mentioned in any of the legislation aimed at supposedly making sports more fair.
What Newsom is parroting, aligns with one of Trump’s recently signed executive orders which is titled ‘Keeping Men Out of Women’s Sports.’
The deeply disturbing and entirely misinformed perspective outlined in this executive order is sold to Americans as a form of protection and privacy for athletes, but in fact guarantees the opposite. Athletes will have to continuously undergo unfair and accusatory situations with no one to defend their position, whether they are trans or actually cisgender. This executive order and by extension, the position now shared by Newsom, actually endanger athletes who are cisgender, by relaxing privacy policies that would allow for investigation and prosecution of athletes who are accused of being trans, such as the Utah teen who was accused of being trans and put in danger by the public statement made by a Utah state school board member named Natalie Cline.
Last year, a more prominent example made headlines across the country regarding Imane Khelif, an Olympic boxer who was attacked with hate speech, conspiracies and accusations regarding her gender. She was exposed to bullying and hate by people who questioned her gender, completely ignoring the fact that she was born a female and has competed as a female for many years.
After her first win in the Paris Olympics where she won the fight against her opponent in 46 seconds, frequent critics of transgender rights, including Elon Musk and J.K. Rowling quickly took the opportunity to weigh in.
The mention of Trump’s lapdog, Musk, sickens me but also brings us full-circle to who is funding this anti-trans machine from the very root of the problem. He is not only Trump’s lapdog, but he’s also a multi-billionaire with too much time on his hands and nothing diplomatic or important to say about trans people. Let us not forget that his villain origin story began when ex-wife and baby mama was rumored to be dating infamous trans WikiLeak-er Chelsea Manning after breaking up with Musk.
Since Trump’s inauguration, four other executive orders have been signed to target trans people and the institutions that support gender-affirming care and provide resources. The unfair and continued attacks on two-spirit, trans, gender nonconforming and intersex people, will not stop us from existing, but it will make it harder for us all to co-exist and thrive in a nation that is sold to the rest of the world as a free country.
Opinions
Trump’s allegiance to Putin is anti-American
Why have evangelicals forsaken their God for a fraudulent ‘savior’ who acts more like Satan in disguise?

Wake up. We’re slowly slip-sliding into a Russian-orchestrated coup.
This goes way beyond the jokey rumors that Russian dictator Vladimir Putin is blackmailing Donald Trump with a secret, compromising ‘pee tape.’ Consider how the U.S. voted in the United Nations with Russia, China and Iran against American supposed ally, Ukraine. Now there’s the shocking Oval Office ambush of Ukrainian President Volodymyr Zelensky by Trump and JD Vance.
As a smirking gaslit affront to Republicans, Trump is performing his excessive allegiance to Putin under the recently installed portrait of former Republican icon, President Ronald Reagan. Once upon a time, Republicans ascribed the fall of the totalitarian Soviet Union to Reagan’s strong, moral, anti-Communist principles.
“Let us be aware that while they preach the supremacy of the State, declare its omnipotence over individual man, and predict its eventual domination of all peoples on the earth, they are the focus of evil in the modern world,” Reagan exclaimed at the 1983 National Association of Evangelicals Convention in Orlando, Florida. He warned against ignoring “the facts of history and the aggressive impulses of an evil empire…thereby remov[ing] yourself from the struggle between right and wrong and good and evil.”
Where are the Republicans who cheered Reagan’s ‘evil empire’ speech now? Why do Republicans plug their ears when historians say Putin wants to restore the glory of the Soviet empire – by any means necessary?
Why do Republicans ignore the fact that former KGB agent Vladimir Putin is a communist.
By the way – where are all the Charlton Heston-loving evangelicals who watched him as Moses and cheered when he shouted from atop Mount Sinai, “Thou shalt have no other gods before me” – the first of God’s Ten Commandments. Look at that garish Golden Calf! It’s something charlatan Trump would feature in his NYC apartment or sell for crypto online.
Why have evangelicals forsaken their God for a fraudulent ‘savior’ who acts more like Satan in disguise?
I confess that I’ve been pissed off at evangelicals since rabidly anti-gay Rev. Jerry Falwell said AIDS was “God’s punishment for homosexuality.” Pastor Peter J. Peters wrote in 1992, “The Death Penalty for Homosexuals is prescribed in the Bible.” Now, Christian Nationals and their allies Trump & Putin make self-determined exceptions to the Ten Commandments while mouthing morality.
Nazi-loving Afrikaner Elon Musk’s unbridled enforcement of Project 2025 is not just about eradicating DEI but also about erasing us. Meanwhile, Democrats have been twisting in the wind trying to find a ‘message’ that will woo workers who believed Trump’s ‘populism.’ Pundits are advising the Democratic Party to stop talking about ‘identities’ and focus on ‘issues’ – with some progressives throwing trans folks under the bus to win votes instead of vigorously standing up for the values of fairness and equality.
Remember when Republicans were vehemently against government telling individuals what they can and cannot do and Democrats extolled the right to Freedom of Expression? Now, ‘identity’ is a slur.
Ask Black women if their race doesn’t impact their access to healthcare. Ask same sex couples if they fear placing a photo of their loved ones on their work desk might get them fired. Ask fundraisers and pollsters and nonprofit organizers if ‘identity’ demographics matter when voting on issues.
But none of this will matter if we don’t actively intervene to stop Trump’s Putin coup. Last week, former Fox Weekend co-host and current U.S. Secretary of Defense Pete Hegseth ordered the U.S. Cyber Command to halt “all planning against Russia,” according to a Feb. 28 report in the cybersecurity publication The Record.
The Recorded Future story reported how Russian state-backed hackers compromised SolarWinds Inc.’s systems and its Orion network management platform in 2023, distributing malware “to thousands of enterprises and government organizations” with “numerous other cyberattacks” discovered later.
“If Hegseth’s order only applies to the armed service members focused on Russia, it will reportedly affect several hundred cybersecurity experts,” though “several thousand personnel could be affected if the guidance also encompasses other teams,” The Report says. “Those other teams focus on tasks such as intelligence analysis and capabilities development.”
“How much more proof do we need that this administration is completely compromised?” Brian Krebs, a cybercrime and security investigative journalist, wrote on infosec.exchange. “There is zero reason for the US to relax any offensive digital actions against Russia. If anything, we should be applying more.”
This is hard. How close we thought we’d come to full equality with Obama, Biden, Hillary and Kamala – only to find, like the Paul Simon song says, “the nearer your destination/The more you’re slip sliding away.”
But we can’t give up. Rather, let’s take inspiration from the “Eyes on the Prize” series: “We Who Believe in Freedom Cannot Rest.”
Conclusion: America has switched sides in the Ukraine-Russian war. Up till now, we supported Ukraine’s existential fight for democracy, knowing they are on the frontlines for the free world.
I want to live & die knowing I fought for freedom.

Major victory for LGBTQ funding in LA County

La marcha LGBTQ+ desafía el silencio en El Salvador

Two new books on dining out LGBTQ-style

Latina Turner comes to Bring It To Brunch

‘White Lotus,’ ‘Severance,’ ‘Andor’ lead Dorian TV Awards noms

I’m a queer Iranian Jew. Why I stand with Israel during this conflict

White House finds Calif. violated Title IX by allowing trans athletes in school sports

Drama unfolds for San Diego Pride ahead of festivities
Two new books on dining out LGBTQ-style
Latina Turner comes to Bring It To Brunch
-
 Viewpoint4 days ago
Viewpoint4 days agoI’m a queer Iranian Jew. Why I stand with Israel during this conflict
-
 Congress4 days ago
Congress4 days agoWhite House finds Calif. violated Title IX by allowing trans athletes in school sports
-
 News5 days ago
News5 days agoDrama unfolds for San Diego Pride ahead of festivities
-
 Books2 days ago
Books2 days agoTwo new books on dining out LGBTQ-style
-
 a&e features3 days ago
a&e features3 days agoLatina Turner comes to Bring It To Brunch
-
 Breaking News2 hours ago
Breaking News2 hours agoMajor victory for LGBTQ funding in LA County
-
 Television3 days ago
Television3 days ago‘White Lotus,’ ‘Severance,’ ‘Andor’ lead Dorian TV Awards noms
-
 El Salvador7 hours ago
El Salvador7 hours agoLa marcha LGBTQ+ desafía el silencio en El Salvador