
AIDS and HIV
March 27, 1983: 1,112 and Counting
Larry Kramer’s call to arms
 If this article doesn’t scare the shit out of you, we’re in real trouble. If this article doesn’t rouse you to anger, fury, rage, and action, gay men may have no future on this earth. Our continued existence depends on just how angry you can get.
If this article doesn’t scare the shit out of you, we’re in real trouble. If this article doesn’t rouse you to anger, fury, rage, and action, gay men may have no future on this earth. Our continued existence depends on just how angry you can get.
I am writing this as Larry Kramer, and I am speaking for myself, and my views are not to be attributed to Gay Men’s Health Crisis.
I repeat: Our continued existence as gay men upon the face of this earth is at stake. Unless we fight for our lives, we shall die. In all the history of homosexuality we have never before been so close to death and extinction. Many of us are dying or already dead.
Before I tell you what we must do, let me tell you what is happening to us.
There are now 1,112 cases of serious Acquired Immune Deficiency Syndrome. When we first became worried, there were only 41. In only twenty-eight days, from January 13th to February 9th [1983], there were 164 new cases – and 73 more dead. The total death tally is now 418. Twenty percent of all cases were registered this January alone. There have been 195 dead in New York City from among 526 victims. Of all serious AIDS cases, 47.3 percent are in the New York metropolitan area.
These are the serious cases of AIDS, which means Kaposi’s sarcoma, Pneumocystis carinii pneumonia, and other deadly infections. These numbers do not include the thousands of us walking around with what is also being called AIDS: various forms of swollen lymph glands and fatigues that doctors don’t know what to label or what they might portend.
The rise in these numbers is terrifying. Whatever is spreading is now spreading faster as more and more people come down with AIDS.
And, for the first time in this epidemic, leading doctors and researchers are finally admitting they don’t know what’s going on. I find this terrifying too – as terrifying as the alarming rise in numbers. For the first time, doctors are saying out loud and up front, “I don’t know.”
For two years they weren’t talking like this. For two years we’ve heard a different theory every few weeks. We grasped at the straws of possible cause: promiscuity, poppers, back rooms, the baths, rimming, fisting, anal intercourse, urine, semen, shit, saliva, sweat, blood, blacks, a single virus, a new virus, repeated exposure to a virus, amoebas carrying a virus, drugs, Haiti, voodoo, Flagyl, constant bouts of amebiasis, hepatitis A and B, syphilis, gonorrhea.
I have talked with the leading doctors treating us. One said to me, “If I knew in 1981 what I know now, I would never have become involved with this disease.” Another said, “The thing that upsets me the most in all of this is that at any given moment one of my patients is in the hospital and something is going on with him that I don’t understand. And it’s destroying me because there’s some craziness going on in him that’s destroying him.” A third said to me, “I’m very depressed. A doctor’s job is to make patients well. And I can’t. Too many of my patients die.”
After almost two years of an epidemic, there still are no answers. After almost two years of an epidemic, the cause of AIDS remains unknown. After almost two years of an epidemic, there is no cure.
Hospitals are now so filled with AIDS patients that there is often a waiting period of up to a month before admission, no matter how sick you are. And, once in, patients are now more and more being treated like lepers as hospital staffs become increasingly worried that AIDS is infectious.
Suicides are now being reported of men who would rather die than face such medical uncertainty, such uncertain therapies, such hospital treatment, and the appalling statistic that 86 percent of all serious AIDS cases die after three years’ time.
If all of this had been happening to any other community for two long years, there would have been, long ago, such an outcry from that community and all its members that the government of this city and this country would not know what had hit them.
Why isn’t every gay man in this city so scared shitless that he is screaming for action? Does every gay man in New York want to die?
Let’s talk about a few things specifically.
Let’s talk about which gay men get AIDS.
No matter what you’ve heard, there is no single profile for all AIDS victims. There are drug users and non-drug users. There are the truly promiscuous and the almost monogamous. There are reported cases of single-contact infection.
All it seems to take is the one wrong fuck. That’s not promiscuity – that’s bad luck.
· Let’s talk about AIDS happening in straight people.
We have been hearing from the beginning of this epidemic that it was only a question of time before the straight community came down with AIDS, and that when that happened AIDS would suddenly be high on all agendas for funding and research and then we would finally be looked after and all would then be well.
I myself thought, when AIDS occurred in the first baby, that would be the breakthrough point. It was. For one day the media paid an enormous amount of attention. And that was it, kids.
There have been no confirmed cases of AIDS in straight, white, non-intravenous-drug-using, middle-class Americans. The only confirmed straights struck down by AIDS are members of groups just as disenfranchised as gay men: intravenous drug users, Haitians, eleven hemophiliacs (up from eight), black and Hispanic babies, and wives or partners of IV drug users and bisexual men.
If there have been – and there may have been – any cases in straight, white, non-intravenous-drug-using, middle-class Americans, the Centers for Disease Control isn’t telling anyone about them. When pressed, the CDC says there are “a number of cases that don’t fall into any of the other categories.” The CDC says it’s impossible to fully investigate most of these “other category” cases; most of them are dead. The CDC also tends not to believe living, white, middle-class male victims when they say they’re straight, or female victims when they say their husbands are straight and don’t take drugs.
Why isn’t AIDS happening to more straights? Maybe it’s because gay men don’t have sex with them.
Of all serious AIDS cases, 72.4 percent are in gay and bisexual men.
· Let’s talk about “surveillance.”
The Centers for Disease Control is charged by our government to fully monitor all epidemics and unusual diseases.
To learn something from an epidemic, you have to keep records and statistics. Statistics come from interviewing victims and getting as much information from them as you can. Before they die. To get the best information, you have to ask the right questions.
There have been so many AIDS victims that the CDC is no longer able to get to them fast enough. It has given up. (The CDC also had been using a questionnaire that was fairly insensitive to the lives of gay men, and thus the data collected from its early study of us have been disputed by gay epidemiologists. The National Institutes of Health is also fielding a very naive questionnaire.)
Important, vital case histories are now being lost because of this cessation of CDC interviewing. This is a woeful waste with as terrifying implications for us as the alarming rise in case numbers and doctors finally admitting they don’t know what’s going on. As each man dies, as one or both sets of men who had interacted with each other come down with AIDS, yet more information that might reveal patterns of transmissibility is not :being monitored and collected and studied. We are being denied perhaps the easiest and fastest research tool available at this moment.
It will require at least $200,000 to prepare a new questionnaire to study the next important question that must be answered: How is AIDS being transmitted? (In which bodily fluids, by which sexual behaviors, in what social environments?)
For months the CDC has been asked to begin such preparations for continued surveillance. The CDC is stretched to its limits and is dreadfully underfunded for what it’s being asked, in all areas, to do.
· Let’s talk about various forms of treatment.
It is very difficult for a patient to find out which hospital to go to or which doctor to go to or which mode of treatment to attempt.
Hospitals and doctors are reluctant to reveal how well they’re doing with each type of treatment. They may, if you press them, give you a general idea. Most will not show you their precise numbers of how many patients are doing well on what and how many failed to respond adequately.
Because of the ludicrous requirements of the medical journals, doctors are prohibited from revealing publicly the specific data they are gathering from their treatments of our bodies. Doctors and hospitals need money for research, and this money (from the National Institutes of Health, from cancer research funding organizations, from rich patrons) comes based on the performance of their work (i.e., their tabulations of their results of their treatment of our bodies); this performance is written up as “papers” that must be submitted to and accepted by such “distinguished” medical publications as the New England Journal of Medicine. Most of these “distinguished” publications, however, will not publish anything that has been spoken of, leaked, announced, or intimated publicly in advance. Even after acceptance, the doctors must hold their tongues until the article is actually published. Dr. Bijan Safai of Sloan-Kettering has been waiting over six months for the New England Journal, which has accepted his interferon study, to publish it. Until that happens, he is only permitted to speak in the most general terms of how interferon is or is not working.
Priorities in this area appear to be peculiarly out of kilter at this moment of life or death.
· Let’s talk about hospitals.
Everybody’s full up, fellows. No room in the inn.
Part of this is simply overcrowding. Part of this is cruel.
Sloan-Kettering still enforces a regulation from pre-AIDS days that only one dermatology patient per week can be admitted to that hospital. (Kaposi’s sarcoma falls under dermatology at Sloan-Kettering.) But Sloan-Kettering is also the second-largest treatment center for AIDS patients in New York. You can be near death and still not get into Sloan-Kettering.
Additionally, Sloan-Kettering (and the Food and Drug Administration) requires patients to receive their initial shots of interferon while they are hospitalized. A lot of men want to try interferon at Sloan-Kettering before they try chemotherapy elsewhere.
It’s not hard to see why there’s such a waiting list to get into Sloan-Kettering.
Most hospital staffs are still so badly educated about AIDS that they don’t know much about it, except that they’ve heard it’s infectious. (There still have been no cases in hospital staff or among the very doctors who have been treating AIDS victims for two years.) Hence, as I said earlier, AIDS patients are often treated like lepers.
For various reasons, I would not like to be a patient at the Veterans Administration Hospital on East 24th Street or at New York Hospital. (Incidents involving AIDS patients at these two hospitals have been reported in news stories in the Native.)
I believe it falls to this city’s Department of Health, under Commissioner David Sencer, and the Health and Hospitals Corporation, under Commissioner Stanley Brezenoff, to educate this city, its citizens, and its hospital workers about all areas of a public health emergency. Well, they have done an appalling job of educating our citizens, our hospital workers, and even, in some instances, our doctors. Almost everything this city knows about AIDS has come to it, in one way or another, through Gay Men’s Health Crisis. And that includes television programs, magazine articles, radio commercials, newsletters, health-recommendation brochures, open forums, and sending speakers everywhere, including – when asked – into hospitals. If three out of four AIDS cases were occurring in straights instead of in gay men, you can bet all hospitals and their staffs would know what was happening. And it would be this city’s Health Department and Health and Hospitals Corporation that would be telling them.
· Let’s talk about what gay tax dollars are buying for gay men.
Now we’re arriving at the truly scandalous. For over a year and a half the National Institutes of Health has been “reviewing” which from among some $55 million worth of grant applications for AIDS research money it will eventually fund.
It’s not even a question of NIH having to ask Congress for money. It’s already there. Waiting. NIH has almost $8 million already appropriated that it has yet to release into usefulness.
There is no question that if this epidemic was happening to the straight, white, non-intravenous-drug-using middle class, it that money would have been put into use almost two years ago, when the first alarming signs of this epidemic were noticed by Dr. Alvin Friedman-Kien and Dr. Linda Laubenstein at New York University Hospital.
During the first two weeks of the Tylenol scare, the United States Government spent $10 million to find out what was happening.
Every hospital in New York that’s involved in AIDS research has used up every bit of the money it could find for researching AIDS while waiting for NIH grants to come through. These hospitals have been working on AIDS for up to two years and are now desperate for replenishing funds. Important studies that began last year, such as Dr. Michael Lange’s at St. Luke’s-Roosevelt, are now going under for lack of money. Important leads that were and are developing cannot be pursued. (For instance, few hospitals can afford plasmapheresis machines, and few patients can afford this experimental treatment either, since few insurance policies will cover the $16,600 bill.) New York University Hospital, the largest treatment center for AIDS patients in the world, has had its grant application pending at NIH for a year and a half. Even if the application is successful, the earliest time that NYU could receive any money would be late summer.
The NIH would probably reply that it’s foolish just to throw money away, that that hasn’t worked before. And, NIH would say, if nobody knows what’s happening, what’s to study?
Any good administrator with half a brain could survey the entire AIDS mess and come up with twenty leads that merit further investigation. I could do so myself. In any research, in any investigation, you have to start somewhere. You can’t just not start anywhere at all.
But then, AIDS is happening mostly to gay men, isn’t it?
All of this is indeed ironic. For within AIDS, as most researchers have been trying to convey to the NIH, perhaps may reside the answer to the question of what it is that causes cancer itself. If straights had more brains, or were less bigoted against gays, they would see that, as with hepatitis B, gay men are again doing their suffering for them, revealing this disease to them. They can use us as guinea pigs to discover the cure for AIDS before it hits them, which most medical authorities are still convinced will be happening shortly in increasing numbers.
(As if it had not been malevolent enough, the NIH is now, for unspecified reasons, also turning away AIDS patients from its hospital in Bethesda, Maryland. The hospital, which had been treating anyone and everyone with AIDS free of charge, now will only take AIDS patients if they fit into their current investigating protocol. Whatever that is. The NIH publishes “papers,” too.)
Gay men pay taxes just like everyone else. NIH money should be paying for our research just like everyone else’s. We desperately need something from our government to save our lives, and we’re not getting it.
· Let’s talk about health insurance and welfare problems.
Many of the ways of treating AIDS are experimental, and many health insurance policies do not cover most of them. Blue Cross is particularly bad about accepting anything unusual.
Many serious victims of AIDS have been unable to qualify for welfare or disability or social security benefits. There are increasing numbers of men unable to work and unable to claim welfare because AIDS is not on the list of qualifying disability illnesses. (Immune deficiency is an acceptable determining factor for welfare among children, but not adults. Figure that one out.) There are also increasing numbers of men unable to pay their rent, men thrown out on the street with nowhere to live and no money to live with, and men who have been asked by roommates to leave because of their illnesses. And men with serious AIDS are being fired from certain jobs.
The horror stories in this area, of those suddenly found destitute, of those facing this illness with insufficient insurance, continue to mount. (One man who’d had no success on other therapies was forced to beg from his friends the $16,600 he needed to try, as a last resort, plasmapheresis.)
· Finally, let’s talk about our mayor, Ed Koch.
Our mayor, Ed Koch, appears to have chosen, for whatever reason, not to allow himself to be perceived by the non-gay world as visibly helping us in this emergency. Repeated requests to meet with him have been denied us. Repeated attempts to have him make a very necessary public announcement about this crisis and public health emergency have been refused by his staff. I sometimes think he doesn’t know what’s going on. I sometimes think that, like some king who has been so long on his throne he’s lost touch with his people, Koch is so protected and isolated by his staff that he is unaware of what fear and pain we’re in. No human being could otherwise continue to be so useless to his suffering constituents. When I was allowed a few moments with him at a party for outgoing Cultural Affairs Commissioner (and Gay Men’s Health Crisis Advisory Board member) Henry Geldzahler, I could tell from his responses that mayor Koch had not been well briefed on AIDS or what is happening in his city. When I started to fill him in, I was pulled away by an aide, who said, “Your time is up.”
I could see our mayor relatively blameless in his shameful.secreting of himself from our need of him in this time of epidemic – except for one fact. Our mayor thinks so little of us that he has assigned as his “liaison” to the gay community a man of such appalling insensitivity to our community and its needs that I am ashamed to say he is a homosexual. His name is Herb Rickman, and for a while our mayor saw fit to have Rickman serve as liaison to the Hasidic Jewish community, too. Hasidic Jews hate gays. Figure out a mayor who would do that to you.
To continue to allow Herb Rickman to represent us in City Hall will, in my view, only bring us closer to death.
When I denounced Rickman at a recent gay Community Council meeting, I received a resounding ovation. He is almost universally hated by virtually every gay organization in New York. Why, then, have we all allowed this man to shit on us so, to refuse our phone calls, to scream at us hysterically, to slam down telephones, to threaten us, to tease us with favors that are not delivered, to keep us waiting hours for an audience, to lie to us – in short, to humiliate us so? He would not do this to black or Jewish leaders. And they would not take it from him for one minute. Why, why, why do we allow him to do it to us? And he, a homosexual!
One can only surmise that our mayor wants us treated this way.
My last attempt at communication with Herb Rickman was on January 23rd [1983], when, after several days of his not returning my phone calls, I wrote to him that the mayor continued to ignore our crisis at his peril. And I state here and now that if Mayor Ed Koch continues to remain invisible to us and to ignore us in this era of mounting death, I swear I shall do everything in my power to see that he never wins elective office again.
Rickman would tell you that the mayor is concerned, that he has established an “Inter-Departmental Task Force” – and, as a member of it, I will tell you that this Task Force is just lip service and a waste of everyone’s time. It hasn’t even met for two months. (Health Commissioner David Sencer had his gallstones out.)
On October 28th, 1982, Mayor Koch was implored to make a public announcement about our emergency. If he had done so then, and if he was only to do so now, the following would be put into action:
1. The community at large would be alerted (you would be amazed at how many people, including gay men, still don’t know enough about the AIDS danger).
2. Hospital staffs and public assistance offices would also be alerted and their education commenced.
3. The country, President Reagan, and the National Institutes of Health, as well as Congress, would be alerted, and these constitute the most important ears of all.
If the mayor doesn’t think it’s important enough to talk up AIDS, none of these people is going to, either.
The Mayor of New York has an enormous amount of power – when he wants to use it. When he wants to help his people. With the failure yet again of our civil rights bill, I’d guess our mayor doesn’t want to use his power to help us.
With his silence on AIDS, the Mayor of New York is helping to kill us.
* * *
I am sick of our electing officials who in no way represent us. I am sick of our stupidity in believing candidates who promise us everything for our support and promptly forget us and insult us after we have given them our votes. Koch is the prime example, but not the only one. Daniel Patrick Moynihan isn’t looking very good at this moment, either. Moynihan was requested by gay leaders to publicly ask Margaret Heckler at her confirmation hearing for Secretary of Health and Human Services if she could be fair to gays in view of her voting record of definite anti-gay bias. (Among other horrors, she voted to retain the sodomy law in Washington, D.C., at Jerry Falwell’s request.) Moynihan refused to ask this question, as he has refused to meet with us about AIDS, despite our repeated requests. Margaret Heckler will have important jurisdiction over the CDC, over the NIH, over the Public Health Service, over the Food and Drug Administration – indeed, over all areas of AIDS concerns. Thank you, Daniel Patrick Moynihan. I am sick of our not realizing we have enough votes to defeat these people, and I am sick of our not electing our own openly gay officials in the first place. Moynihan doesn’t even have an openly gay person on his staff, and he represents the city with the largest gay population in America.
I am sick of closeted gay doctors who won’t come out to help us fight to rectify any of what I’m writing about. Doctors – the very letters “M.D.” – have enormous clout, particularly when they fight in groups. Can you imagine what gay doctors could accomplish, banded together in a network, petitioning local and federal governments, straight colleagues, and the American Medical Association? I am sick of the passivity or nonparticipation or halfhearted protestation of all the gay medical associations (American Physicians for Human Rights, Bay Area Physicians for Human Rights, Gay Psychiatrists of New York, etc., etc.), and particularly our own New York Physicians for Human Rights, a group of 175 of our gay doctors who have, as a group, done nothing. You can count on one hand the number of our doctors who have really worked for us.
I am sick of the Advocate, one of this country’s largest gay publications, which has yet to quite acknowledge that there’s anything going on. That newspaper’s recent AIDS issue was so innocuous you’d have thought all we were going through was little worse than a rage of the latest designer flu. And their own associate editor, Brent Harris, died from AIDS. Figure that one out.
With the exception of the New York Native and a few, very few, other gay publications, the gay press has been useless. If we can’t get our own papers and magazines to tell us what’s really happening to us, and this negligence is added to the negligent non-interest of the straight press (The New York Times took a leisurely year and a half between its major pieces, and the Village Voice took a year and a half to write anything at all), how are we going to get the word around that we’re dying? Gay men in smaller towns and cities everywhere must be educated, too. Has the Times or the Advocate told you that twenty-nine cases have been reported from Paris?
I am sick of gay men who won’t support gay charities. Go give your bucks to straight charities, fellows, while we die. Gay Men’s Health Crisis is going crazy trying to accomplish everything it does – printing and distributing hundreds of thousands of educational items, taking care of several hundred AIDS victims (some of them straight) in and out of hospitals, arranging community forums and speakers all over this country, getting media attention, fighting bad hospital care, on and on and on, fighting for you and us in two thousand ways, and trying to sell 17,600 Circus tickets, too. Is the Red Cross doing this for you? Is the American Cancer Society? Your college alumni fund? The United Jewish Appeal? Catholic Charities? The United Way? The Lenox Hill Neighborhood Association, or any of the other fancy straight charities for which faggots put on black ties and dance at the Plaza? The National Gay Task Force – our only hope for national leadership, with its new and splendid leader, Virginia Apuzzo – which is spending more and more time fighting for the AIDS issue, is broke. Senior Action in a Gay Environment and Gay Men’s Health Crisis are, within a few months, going to be without office space they can afford, and thus will be out on the street. The St. Mark’s Clinic, held together by some of the few devoted gay doctors in this city who aren’t interested in becoming rich, lives in constant terror of even higher rent and eviction. This community is desperate for the services these organizations are providing for it. And these organizations are all desperate for money, which is certainly not coming from straight people or President Reagan or Mayor Koch. (If every gay man within a 250-mile radius of Manhattan isn’t in Madison Square Garden on the night of April 30th to help Gay Men’s Health Crisis make enough money to get through the next horrible year of fighting against AIDS, I shall lose all hope that we have any future whatsoever.)
I am sick of closeted gays. It’s 1983 already, guys, when are you going to come out? By 1984 you could be dead. Every gay man who is unable to come forward now and fight to save his own life is truly helping to kill the rest of us. There is only one thing that’s going to save some of us, and this is numbers and pressure and our being perceived as united and a threat. As more and more of my friends die, I have less and less sympathy for men who are afraid their mommies will find out or afraid their bosses will find out or afraid their fellow doctors or professional associates will find out. Unless we can generate, visibly, numbers, masses, we are going to die.
I am sick of everyone in this community who tells me to stop creating a panic. How many of us have to die before you get scared off your ass and into action? Aren’t 195 dead New Yorkers enough? Every straight person who is knowledgeable about the AIDS epidemic can’t understand why gay men aren’t marching on the White House. Over and over again I hear from them, “Why aren’t you guys doing anything?” Every politician I have spoken to has said to me confidentially, “You guys aren’t making enough noise. Bureaucracy only responds to pressure.”
I am sick of people who say “it’s no worse than statistics for smokers and lung cancer” or “considering how many homosexuals there are in the United States, AIDS is really statistically affecting only a very few.” That would wash if there weren’t 164 cases in twenty-eight days. That would wash if case numbers hadn’t jumped from 41 to 1,112 in eighteen months. That would wash if cases in one city – New York – hadn’t jumped to cases in fifteen countries and thirty-five states (up from thirty-four last week). That would wash if cases weren’t coming in at more than four a day nationally and over two a day locally. That would wash if the mortality rate didn’t start at 38 percent the first year of diagnosis and climb to a grotesque 86 percent after three years. Get your stupid heads out of the sand, you turkeys!
I am sick of guys who moan that giving up careless sex until this blows over is worse than death. How can they value life so little and cocks and asses so much? Come with me, guys, while I visit a few of our friends in Intensive Care at NYU. Notice the looks in their eyes, guys. They’d give up sex forever if you could promise them life.
I am sick of guys who think that all being gay means is sex in the first place. I am sick of guys who can only think with their cocks.
I am sick of “men” who say, “We’ve got to keep quiet or they will do such and such.” They usually means the straight majority, the “Moral” Majority, or similarly perceived representatives of them. Okay, you “men” – be my guests: You can march off now to the gas chambers; just get right in line.
We shall always have enemies. Nothing we can ever do will remove them. Southern newspapers and Jerry Falwell’s publications are already printing editorials proclaiming AIDS as God’s deserved punishment on homosexuals. So what? Nasty words make poor little sissy pansy wilt and die?
And I am very sick and saddened by every gay man who does not get behind this issue totally and with commitment – to fight for his life.
* * *
I don’t want to die. I can only assume you don’t want to die. Can we fight together?
For the past few weeks, about fifty community leaders and organization representatives have been meeting at Beth Simchat Torah, the gay synagogue, to prepare action. We call ourselves the AIDS Network. We come from all areas of health concern: doctors, social workers, psychologists, psychiatrists, nurses; we come from Gay Men’s Health Crisis, from the National Gay Health Education Foundation, from New York Physicians for Human Rights, the St. Mark’s Clinic, the Gay Men’s Health Project; we come from the gay synagogue, the Gay Men’s Chorus, from the Greater Gotham Business Council, SAGE, Lambda Legal Defense, Gay Fathers, the Christopher Street Festival Committee, Dignity, Integrity; we are lawyers, actors, dancers, architects, writers, citizens; we come from many component organizations of the Gay and Lesbian Community Council.
We have a leader. Indeed, for the first time our community appears to have a true leader. Her name is Virginia Apuzzo, she is head of the National Gay Task Force, and, as I have said, so far she has proved to be magnificent.
The AIDS Network has sent a letter to Mayor Koch. It “contains twelve points that are urged for his consideration and action.”
This letter to Mayor Koch also contains the following paragraph:
It must be stated at the outset that the gay community is growing increasingly aroused and concerned and angry. Should our avenues to the mayor of our city and the members of the Board of Estimate not be available, it is our feeling that the level of frustration is such that it will manifest itself in a manner heretofore not associated with this community and the gay population at large. It should be stated, too, at the outset, that as of February 25th, there were 526 cases of serious AIDS in New York’s metropolitan area and 195 deaths (and 1,112 cases nationally and 418 deaths) and it is the sad and sorry fact that most gay men in our city now have close friends and lovers who have either been stricken with or died from this disease. It is against this background that this letter is addressed. It is this issue that has, ironically, united our community in a way not heretofore thought possible.
Further, a number of AIDS Network members have been studying civil disobedience with one of the experts from Dr. Martin Luther King’s old team. We are learning how. Gay men are the strongest, toughest people I know. We are perhaps shortly to get an opportunity to show it.
I’m sick of hearing that Mayor Koch doesn’t respond to pressures and threats from the disenfranchised, that he walks away from confrontations. Maybe he does. But we have tried to make contact with him, we are dying, so what other choice but confrontation has he left us?
I hope we don’t have to conduct sit-ins or tie up traffic or get arrested. I hope our city and our country will start to do something to help start saving us. But it is time for us to be perceived for what we truly are: an angry community and a strong community, and therefore a threat. Such are the realities of politics. Nationally we are 24 million strong, which is more than there are Jews or blacks or Hispanics in this country.
I want to make a point about what happens if we don’t get angry about AIDS. There are the obvious losses, of course: Little of what I’ve written about here is likely to be rectified with the speed necessary to help the growing number of victims. But something worse will happen, and is already happening. Increasingly, we are being blamed for AIDS, for this epidemic; we are being called its perpetrators, through our blood, through our “promiscuity,” through just being the gay men so much of the rest of the world has learned to hate. We can point out until we are blue in the face that we are not the cause of AIDS but its victims, that AIDS has landed among us first, as it could have landed among them first. But other frightened populations are going to drown out these truths by playing on the worst bigoted fears of the straight world, and send the status of gays right back to the Dark Ages. Not all Jews are blamed for Meyer Lansky, Rabbis Bergman and Kahane, or for money-lending. All Chinese aren’t blamed for the recent Seattle slaughters. But all gays are blamed for John Gacy, the North American Man/Boy Love Association, and AIDS.
Enough. I am told this is one of the longest articles the Native has ever run. I hope I have not been guilty of saying ineffectively in five thousand words what I could have said in five: we must fight to live.
I am angry and frustrated almost beyond the bound my skin and bones and body and brain can encompass. My sleep is tormented by nightmares and visions of lost friends, and my days are flooded by the tears of funerals and memorial services and seeing my sick friends. How many of us must die before all of us living fight back?
I know that unless I fight with every ounce of my energy I will hate myself. I hope, I pray, I implore you to feel the same.
I am going to close by doing what Dr. Ron Grossman did at GMHC’s second Open Forum last November at Julia Richman High School. He listed the names of the patients he had lost to AIDS. Here is a list of twenty dead men I knew:
Nick Rock
Rick Wellikoff
Jack Nau
Shelly
Donald Krintzman
Jerry Green
Michael Maletta
Paul Graham
Toby
Harry Blumenthal
Stephen Sperry
Brian O’Hara
Barry
David
Jeffrey Croland
Z.
David Jackson
Tony Rappa
Robert Christian
Ron Doud
And one more, who will be dead by the time these words appear in print.
If we don’t act immediately, then we face our approaching doom.
* * *
Volunteers Needed for Civil Disobedience
It is necessary that we have a pool of at least three thousand people who are prepared to participate in demonstrations of civil disobedience. Such demonstrations might include sit-ins or traffic tie-ups. All participants must be prepared to be arrested. I am asking every gay person and every gay organization to canvass all friends and members and make a count of the total number of people you can provide toward this pool of three thousand.
Let me know how many people you can be counted on providing. Just include the number of people; you don’t have to send actual names – you keep that list yourself. And include your own phone numbers. Start these lists now.
L.K.
AIDS and HIV
Aging with HIV: The Latino Commission on AIDS honors National Latino Older Adults & HIV/AIDS Awareness Day
From powerful personal stories to Mamdani’s mayoral proclamation honoring the Latino Commission on AIDS, National Latino Older Adults & HIV/AIDS Awareness Day delivers a necessary reminder that aging with HIV is about not just surviving but thriving

I recently had the privilege of attending the National Latino Older Adults & HIV/AIDS Awareness Day event hosted by the Latino Commission on AIDS, and I was reminded that conversations about HIV must continue to evolve alongside the people living with it. The event brought together advocates, healthcare professionals, community leaders, and long-term survivors to recognize the growing population of older Latino adults living with HIV. It was both a celebration of resilience and an honest acknowledgment of the challenges that still exist. As treatments continue to improve and people with HIV are living longer, it’s important for our conversations to move past survival and focus on what it truly means to age with dignity, purpose, and community.
One major win that I’d be remiss to not share with you was the recognition of the Latino Commission on AIDS through an official proclamation from New York City Mayor Zohran Mamdani. The proclamation honored the Commission’s decades of advocacy, education, and leadership in improving the lives of Latinos affected by HIV/AIDS. It was a fitting tribute to an organization that has consistently worked to combat stigma while expanding access to culturally competent care throughout New York City and beyond.
Director of Aging Initiatives Luis Nava Molero delivered one of the day’s most significant speeches. Rather than focusing solely on statistics, he spoke from personal experience about what it means to grow older while living with HIV. His words were a reminder that behind every diagnosis is a very human story.
“For many people, HIV is a statistic, a diagnosis, or a chapter in history. For me, and for so many others in this room, HIV is a lifetime.”

For those who have lived through the epidemic, HIV is so much more than a diagnosis. It is a journey marked by loss, perseverance, and hope. Nava Molero reflected on the friends who should still be here today, people whose lives were cut short before lifesaving treatments were made available. Remembering them, he said, is both a gift and a responsibility.
Nava Molero also spoke honestly about the realities of aging with HIV, acknowledging that many long-term survivors are managing many other health conditions alongside the virus. Yet his message was not one of hopelessness.
“One of the greatest lessons I have learned is that aging is not simply about growing older. It is about continuing to find purpose.”
Purpose becomes an important part of healthy aging, regardless of someone’s HIV status. Through his work with the Latino Commission on AIDS, Nava Molero continues the legacy of Dennis de León, whose vision centered on ensuring Latino communities were respected and empowered to speak for themselves.
This year’s theme, “Our Health, Our Voice, Our Future,” served as the framework for many of the day’s discussions. Nava Molero reminded attendees that health extends beyond medical care. “Our health is more than our medical condition. It includes our emotional well-being, our relationships, our dignity, and our hope.”
Those words reflect an important shift in how we think about HIV care today. Medical treatment remains paramount, but so does addressing loneliness, mental health, discrimination, and access to supportive services.
Rafael Romero of the Translatina Network expanded that conversation by emphasizing the unique experiences of transgender and gender-nonconforming older adults living with HIV.
“This day reminds us that aging with HIV is not just about living longer, but about thriving,” Romero said. He addressed the ongoing barriers many continue to deal with, like discrimination, social isolation, and limited access to culturally and linguistically appropriate healthcare. His remarks emphasized that equity has to include everyone, particularly those whose identities often put them at the intersection of multiple forms of discrimination.
Romero concluded his speech by reaffirming a commitment to “building inclusive communities where all older adults living with HIV, including transgender and gender-nonconforming individuals, are seen and supported, with the tools they need to thrive, not just survive.”
That message hit home on one of the strongest themes throughout the event: healthcare must be culturally competent and accessible if we hope to eliminate disparities.

Another significant topic was the reminder that folks who take HIV medication consistently and maintain an undetectable viral load cannot sexually transmit the virus, a fact summarized by the now widely recognized message: Undetectable equals Untransmittable, U=U. This scientific breakthrough continues to reduce stigma while offering hope for future generations.
Perhaps the most powerful part of the speech focused not on medicine, but on mindset.
“Hope is something we choose every day. Dreams do not have an expiration date. Purpose does not retire.” These words serve as a reminder that aging is not defined by years lived, but by the opportunities we continue to create for ourselves and others along the way.
Mental health also emerged as a central topic throughout the morning. Several speakers encouraged attendees to recognize their emotions, remain connected to supportive communities, and seek help when needed. As Nava Molero perfectly stated, “Asking for help is not a sign of weakness. It is an act of strength.” Whether someone is living with HIV, managing another chronic illness, or navigating the challenges of aging, reaching out for support must always be viewed as an act of courage rather than vulnerability.
Leaving the event, I found myself thinking less about statistics and more about people. I thought about the advocates who refused to give up during the darkest years of the epidemic. I thought about the long-term survivors who continue to educate, mentor, and inspire others. I thought about the younger generations who benefit from decades of advocacy and scientific progress.
National Latino Older Adults & HIV/AIDS Awareness Day reminds us that there is still work to do. Stigma continues to exist. Health disparities remain. Too many older adults still experience isolation or barriers to care. Yet events like this demonstrate what is possible when organizations, healthcare providers, policymakers, and community members come together with a shared purpose.
The Latino Commission on AIDS has spent decades ensuring that Latino communities affected by HIV are not overlooked. Mamdani’s mayoral proclamation honoring the Latino Commission on AIDS’ work was a very real acknowledgment of this enduring commitment, but perhaps the greatest recognition came from the people gathered in the room, folks whose lives have been touched, changed, and strengthened through its advocacy.
As the event concluded, one message rang hard. Aging with HIV is not just about adding years to life. It is about ensuring that those years are lived with good health, dignity, and community. This is a goal worth pursuing, not only on National Latino Older Adults & HIV/AIDS Awareness Day, but every damn day.
For more information, head to www.latinoaids.org.
AIDS and HIV
45 years later…: Advocate Karl Schmid on why HIV is far from over
HIV may no longer be a death sentence, but Karl Schmid explains why complacency could impact decades of painstaking progress

When we think of Pride, our minds go to bright colors, music, and celebration – and rightfully so. But we also must acknowledge our history of resilience, activism, and lives forever changed by the HIV/AIDS epidemic. This year marks 45 years since the first reported cases of AIDS, a milestone that serves as both a testament to extraordinary scientific progress as well as a reminder that the work is far from finished. While HIV is no longer the death sentence it once was, stigma, misinformation, and inequitable access to care continue to impact the lives of millions around the world.
Few people understand the intersection of progress and persistence better than Karl Schmid. A journalist, advocate, and founder of Plus Life Media, Schmid has spent years using his own lived experience to challenge misconceptions about HIV and amplify the voices of those living with it. In our convo, Schmid reflects on coming out as HIV-positive, why society still struggles to talk openly about stigma, the life-changing impact of U=U, and why honoring the past is about making sure the future arrives for everyone.
This Pride Month marks 45 years since the beginning of the AIDS epidemic. What emotions come up for you when you reflect on this milestone?
It’s a mixed bag, really. On one hand, I feel incredibly grateful and proud. The progress we’ve made over the last 45 years is nothing short of remarkable. Thanks to extraordinary advances in science and medicine, I can expect to live a long, healthy life so long as I remain undetectable, which also means I can’t transmit HIV to a sexual partner. The fact that HIV has gone from being a death sentence to a manageable chronic condition within my lifetime is extraordinary, and something I never take for granted.
On the other hand, sadness, anxiety, and even anger bubble up too. We’re 45 years into this epidemic, and we still don’t have a cure. We still don’t have equitable access to prevention, treatment, and care for everyone who needs it. And we’re living through a moment where some of the hard-fought gains we’ve made are not only being threatened, but in some cases actively rolled back.
What’s particularly frustrating is the growing perception that HIV is “solved” and no longer requires the same level of attention, investment, or urgency. The reality is that millions of people around the world still depend on ongoing research, access to treatment, and support services. Those aren’t luxuries. They’re lifelines.
So when I reflect on this milestone, I feel proud of how far we’ve come, grateful for the people who got us here, and determined not to take any of that progress for granted.
For younger LGBTQ+ folks who did not live through the early days of the epidemic, what is most important for them to know and understand about that time in history?
That HIV didn’t become one of the deadliest epidemics in modern history simply because of a virus. It became what it was because of stigma, discrimination, political inaction, and the belief by many that the people most affected weren’t worth fighting for.
Millions of people died, and for far too long, those in positions of power failed to respond with the urgency the crisis demanded. There was a sense among many that because HIV was primarily affecting gay men, people who used drugs, and other marginalized communities, it wasn’t really their problem. That’s the lesson I hope younger people understand.
The progress we’ve made didn’t happen automatically. It happened because people organized, protested, advocated, cared for one another, and demanded better. Every breakthrough in treatment, every advancement in prevention, every right we’ve secured came from people refusing to accept the status quo. I get angry when I hear people say, “HIV isn’t really something we need to think about anymore.” We are incredibly fortunate to have effective treatment and prevention tools today, but complacency is dangerous. The moment we stop paying attention, stop advocating, or assume the work is done, we risk losing ground.
History shows us what can happen when society decides a problem only belongs to someone else. That’s a lesson that extends far beyond HIV.
What was the response like after you came out as HIV-positive, personally, professionally, or otherwise?
I was incredibly fortunate to have an amazingly supportive family. My parents, my brothers, my extended family, and my close circle of friends were all loving and supportive from day one. Their first concern was simply making sure I was OK. I realize what a position of privilege I sit in to be able to say that.
Professionally, it was a very different story. I kept my HIV status private for 10 years because I was afraid. I was afraid it would affect my career, my ability to work in television, and ultimately the goals and dreams I had for myself. That fear wasn’t based on science. It was based on stigma.
When I finally did speak publicly about living with HIV, the response from my professional circles was, for the most part, incredibly positive. But who’s to say what conversations happened behind closed doors that I wasn’t privy to? Who knows what speaking publicly about my HIV status meant for opportunities that may have come my way but were perhaps reconsidered because of how it might make an organization look? We’ll never know.
What I do know is that holding that secret for so long did more damage to me than the possibility of losing out on jobs or opportunities ever did. The internalized stigma I carried around was heavy. It affected how I saw myself, how I valued myself, and what I believed I was capable of. Even today, that’s something I continue to work on. HIV is a virus. The stigma surrounding it is often much harder to overcome.
Through your work with Plus Life Media, you’ve focused on education and combatting stigma. What conversations about HIV do you think society is still avoiding?
Honestly, I think society is still avoiding conversations about people living with HIV. We’re fairly comfortable talking about HIV in abstract terms. We’ll talk about statistics, research, prevention, treatment, and public health outcomes. Those conversations are important. But we’re often far less comfortable talking about the lived experience of someone who has HIV.
We’re still not having enough honest conversations about stigma. About what it feels like to disclose your status to a potential partner. About the fear some people feel when they’re first diagnosed. About the mental health challenges that can come with carrying stigma for years or even decades. About the fact that many people living with HIV continue to face judgment, including within the LGBTQ+ community itself.
I also think we’re avoiding the conversation that HIV is not over. The headlines have moved on, and because treatment and prevention have improved so dramatically, many people assume the crisis has been solved. But millions of people around the world are still living with HIV, millions more remain vulnerable to acquiring it, and access to prevention, treatment, and care remains wildly unequal depending on where you live.
Ultimately, I think we’re still avoiding the most important conversation of all: how we treat people living with HIV. Science has done its job. We know HIV cannot be sexually transmitted by someone who is undetectable. We know people living with HIV can live long, healthy lives. The question now is whether society is willing to catch up to the science.
HIV treatment and prevention have advanced exponentially over the past few decades. What developments give you the most hope?
The recent approval of Yeztugo from Gilead Sciences is a phenomenal breakthrough. Study after study has shown just how effective it is at preventing HIV through sexual transmission, and the idea that someone can receive just two injections a year for HIV prevention is pretty remarkable when you stop and think about it.
I also know that the amazing folks at Gilead are working with Merck on a potential once-weekly HIV treatment pill. As someone living with HIV, that’s the kind of innovation that gets me excited. Anything that makes prevention and treatment easier and more accessible for people is a good thing.
Beyond specific medications, what gives me hope is knowing there are people and organizations out there dedicating their lives to finding a cure and improving the lives of people living with HIV. They’re not giving up, and they’re not walking away from this work just because funding is being threatened or public trust in science is under attack.
Seeing thousands of young activists show up at AIDS Walks, speak out against cuts to HIV programs, advocate for LGBTQ+ rights, and get involved in their communities gives me enormous hope too. The science gives me hope. The people refusing to stop pushing it forward give me hope, too.
The concept of U=U (Undetectable = Untransmittable) has been major for many people living with HIV. How has that message impacted folks, and why is it still not universally understood?
U=U is one of the most important developments in the history of HIV. Not only because of what it means scientifically, but because of what it means emotionally and psychologically for people living with HIV. U=U has given millions of people their lives back. It means that a person living with HIV who is on treatment and maintains an undetectable viral load cannot sexually transmit the virus. That’s extraordinary.
For generations, people living with HIV carried the fear that they might pass the virus on to someone they loved. U=U changed that. It fundamentally changed how many people living with HIV see themselves, their relationships, and their futures.
We’re also continuing to learn more about other areas, including pregnancy and breastfeeding, with growing evidence and guidance from organizations like the World Health Organization helping to further inform those conversations.
The one caveat, of course, is that U=U only works if someone has access to treatment and is able to maintain an undetectable viral load. That’s why ensuring people have access to testing, treatment, and ongoing care remains so important.
As for why it still isn’t universally understood, I think there are two reasons. The first is stigma. HIV has carried so much fear and misinformation for so long that many people simply haven’t caught up with the science. The second is that old messages stick. Many people still think about HIV the way it was talked about in the 1980s and 1990s, not the way we understand it today. The science has evolved dramatically. Public understanding hasn’t always kept pace.
That’s why conversations about U=U remain so important. It’s not just a scientific message. It’s a message of freedom, dignity, and hope for people living with HIV.
How does HIV stigma intersect with other forms of discrimination like homophobia, racism, and social inequality?
HIV stigma rarely exists on its own. More often than not, it piles on top of other forms of discrimination that people are already experiencing. If you’re LGBTQ+, if you’re a person of color, if you’re living in poverty, if you’re dealing with addiction, if you’re undocumented, if you’re trans, those challenges don’t suddenly disappear because HIV enters the picture. In many cases, they become even harder to navigate.
What I’ve seen over and over again is that the people carrying the heaviest load are often asked to carry even more. If you’re already facing discrimination because of your race, your sexuality, your gender identity, your immigration status, or your financial situation, an HIV diagnosis can add another layer of judgment and stigma on top of everything else.
If someone is afraid to seek care because they’re worried about being judged for being gay, or trans, or because of the color of their skin, or because they can’t afford treatment, that’s not just an HIV issue. That’s a much bigger issue.
That’s why some people can access prevention, treatment, and care with relative ease, while others face obstacle after obstacle. It’s not because the science works differently for them. It’s because life is often harder for them before HIV even enters the picture.
That’s why ending HIV isn’t just about better medicine. It’s also about creating a world where people are treated with dignity, respect, and compassion regardless of who they are or where they come from.
You hosted and executive-produced HIV Unwrapped, a project that merged fashion, science, and narrative. Why do you think creative storytelling can be such an effective route for HIV education?
Because facts inform people. Stories move people. Most people aren’t going to remember a statistic, a scientific paper, or a PowerPoint slide. They’re going to remember how someone made them feel. That’s why storytelling is so powerful.
One of the things HIV Unwrapped did and continues to do so beautifully was take science and turn it into something human. Suddenly, you’re not talking about data points or clinical outcomes. You’re talking about real people, real experiences, and real lives.
At the end of the day, HIV isn’t a science story. It’s a human story. Science is how we end HIV. Storytelling is how we get people to care enough to help us do it.
What did you learn from the researchers, advocates, and people living with HIV who participated in that project?
What I learned is that we’re probably not as different as we like to think we are. On paper, a scientist and a fashion design student don’t appear to have much in common. But watching these relationships develop throughout the project was fascinating. Once they started talking, they quickly realized they were both driven by curiosity, creativity, problem-solving, and a desire to make a positive impact.
That was one of the most rewarding parts of HIV Unwrapped for me. Watching people from completely different worlds come together, learn from one another, and create something neither could have created alone. At a time when society often feels divided, it was a powerful reminder that people have far more in common than what separates them. I found that incredibly inspiring and hopeful.
How can LGBTQ+ communities honor the history of HIV/AIDS while also celebrating progress this Pride (and all) season(s)?
By doing both at the same time. I don’t think honoring the history of HIV/AIDS and celebrating progress are mutually exclusive. In fact, I think one makes the other possible. We can celebrate the fact that people living with HIV are living long, healthy lives. We can celebrate advances in treatment and prevention. We can celebrate how far the LGBTQ+ community has come.
But we should also remember that none of it happened by accident. The rights, freedoms, medical breakthroughs, and opportunities many of us enjoy today exist because previous generations fought for them, often at tremendous personal cost. Many of those people aren’t here to celebrate that progress with us.
So enjoy Pride. Celebrate. Have fun. Be loud. Be joyful. But take a moment to learn the history, honor the people who came before us, and recognize that the best way to respect their legacy is to keep moving the work forward.
For somebody reading this interview who may have recently been diagnosed with HIV, what would you most want them to hear this Pride Month?
First of all, it’s OK to be pissed off. It’s OK to cry, scream, yell, throw things, have a tantrum, and ask, “Why me?” I think most of us have done some version of that after getting diagnosed. But here’s the thing. HIV doesn’t care.
At some point, whether it’s a day later, a week later, or a month later, you’ve got to pick yourself up, dust yourself off, and decide what happens next. The good news is that the future you’re probably imagining right now is almost certainly worse than the reality you’re actually facing.
You’re going to be able to live a long, healthy life. You’re going to fall in love. You’re going to have sex. You’re going to travel. You’re going to have a career. You’re going to make plans for the future. You’re going to do all the things you thought you might not get to do when you first heard those words.
And one day you’ll look back and realize that while HIV became part of your story, it never got to write the whole thing. So feel whatever you need to feel. Then get into care, take your meds, learn about U=U, and get on with living your life. Because HIV is a diagnosis. It’s not a character flaw.
Check out PlusLifeMedia.com
AIDS and HIV
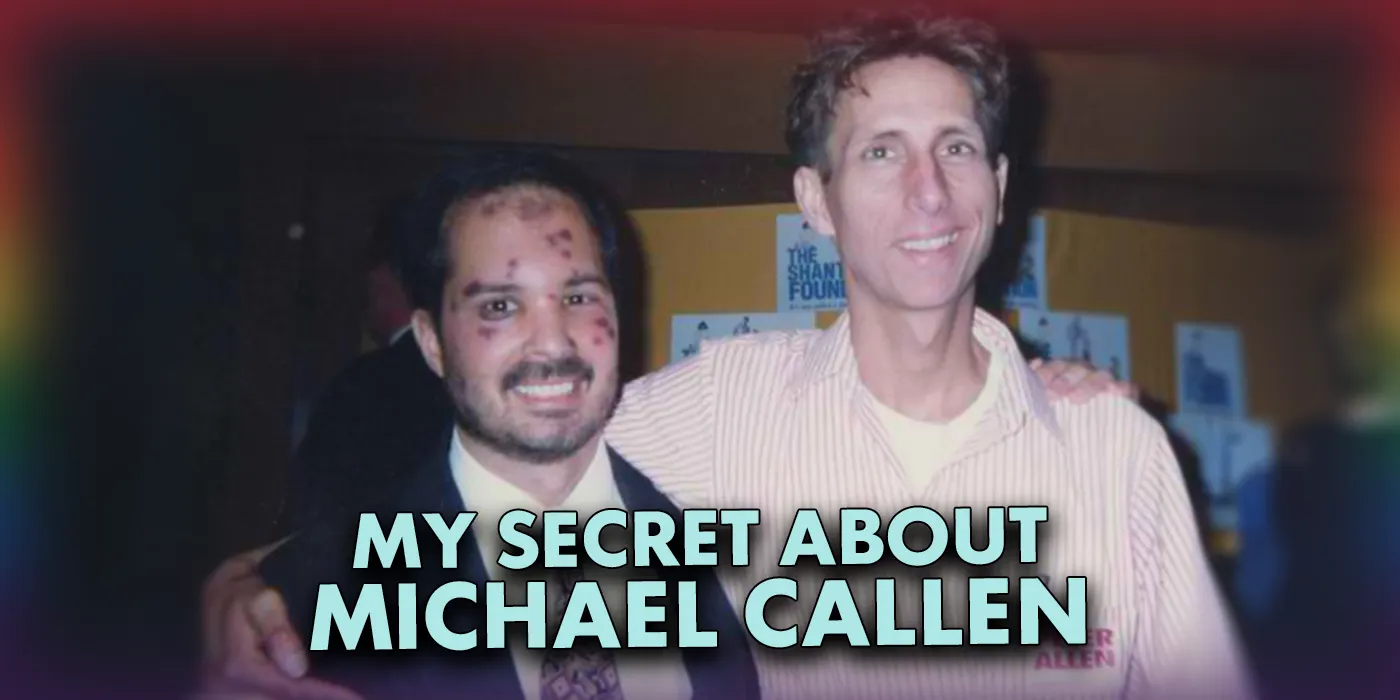
AIDS at 45: My secret about Michael Callen
My PTSD is acting up, reminding me about how much I miss living intensely.
I’ve only shared this secret once – in January 1994 with gay Jungian psychologist Don Kilhefner, who offered to help when he found me trembling and confused outside an AA meeting at Fairfax and Fountain in West Hollywood.
I was falling apart. My friend Michael Callen had just died a few weeks earlier, and now, with the Northridge earthquake, I’d lost my balance. I couldn’t trust the ground I stood on. I literally concentrated on taking every step.
I blurted out how I felt like I’d failed Michael. He lived down the street from me, was a fellow writer for Genre Magazine, and, having become friends, I was one of his care providers.
On a trip back home from a doctor’s appointment, he asked me if I would help him die. We’d talked about death before, so I wasn’t surprised. And because I felt guilty about refusing to help an AA buddy get drunk before he died, I said yes.
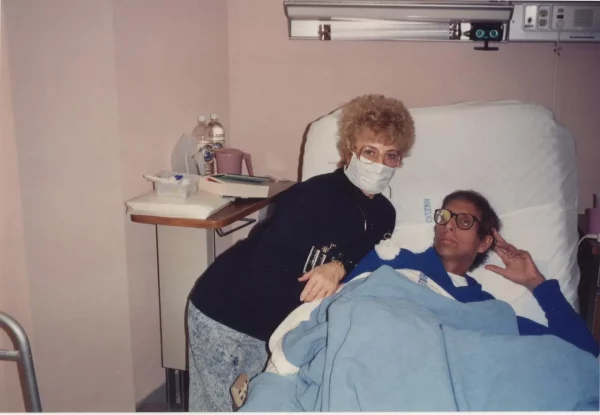
We made a plan. Over the AIDS years, many of us had learned when and how to “punch the bolo” – slang for pressing the button on a pain pump that delivered morphine into a patient’s blood system. Michael would organize a Christmas party in his room at Midway Hospital, and when he was ready, he’d say goodbye, ask people to leave, and I’d punch the bolo.
And that’s what we did. Michael nodded to me, said he was ready, and I punched the bolo – and nothing happened.

We were shocked. Michael had a pained “Oh, NO!” look on his face. He was ready! It was time! Eight months earlier, with KS in his lungs, he sang “Love Don’t Need a Reason” at the 1993 March on Washington and proudly held that last note longer than Barbra Streisand. Recently, with KS turning his right leg into a cement pound of purple flesh, we’d written his goodbye to the community for Genre. He was done.

I punched again. Nothing. Panicked, I ran to the nurse’s office and said told a nurse the morphine wasn’t coming through. She came and checked the pump. It had already dispensed the medication and was on a timer. But we can’t wait, I said, with Michael nodding in his bed. She turned and left.
I clutched Michael’s arm as Dr. Robbie Jenkins came into the room. He was a gay, well-liked AIDS doctor. We trusted him. He flicked the tube and checked everything as I pleaded with him – Michael was ready and wanted to die. Robbie – whom I knew through author Paul Monette – pulled me aside and explained that assisted suicide was illegal, and while he understood, Michael was too famous for him to let that happen here, now.
Robbie apologized, then left. He’d get in trouble and maybe even lose his license if anyone even knew he was having this conversation with me.
Michael was devastated. But for some reason, he seemed to surrender and breathe and decided he was going to die when he was going to die. Meanwhile, let’s get back to Christmas.
I was devastated, too, apologizing, apologizing, apologizing. Michael told me to let it go. It was alright. It wasn’t, and I never forgot.
Michael died two days later. I helped him reconcile with this family in Hamilton, Ohio, before he died. That caused some controversy – but I didn’t care.
He stirred out of his coma when I put the phone to his ear as he listened to his brother Barry, his father Clifford, and his mother, Barbara, say goodbye. A tear rolled down the right side of his cheek as he managed to say, “I love you, too,” to his mother. He was done and fell back into a coma, letting go about two hours later. He was 38.
Michael Callen was famous. And important. And he saved a lot of lives through his AIDS self-empowerment messages, his book Surviving AIDS, and originating “safer sex” through How to Have Sex in an Epidemic: One Approach with Richard Berkowitz and their doctor and mentor, Dr. Joseph Sonnabend.
And Michael was a singer. And a feminist. And a friend. And that’s the heartbreak for so many of us who find ourselves longing for the love we shared, for triumphing over the challenges to our humanity, to the spiritual vanguard we became.
“Living with AIDS is like living in wartime, only in the twilight zone,” Michael once said in a speech. “A majority of your fellow citizens don’t seem to realize there’s a war going on, don’t hear the bombs dropping, the shells whizzing past your head, don’t have to step over the dead bodies of friends and loved ones.”
But we knew. Sometimes in the pain and darkness, a hand will clasp another hand and squeeze for a moment. Life. Recognition. Dignity. And a self-empowering choice we honored with love.
On February 10, 1993, I introduced Michael to the remarkable and kind Daniel P. Warner, founder of LA Shanti, the first AIDS organization in LA. Michael was there to accept an award during LA Shanti’s Peter Allen Memorial Tribute Concert at UCLA. Among the many stars there that night was Miss America 1993, Leanza Cornett, who served as Danny’s date. Danny died on his 38th birthday on June 14, 1993.
I may have failed Michael when he expected and needed my help. But I also promised to never forget him – and I haven’t. And that memory is evidence of our shared humanity.
The night of the tribute, Michael sang “Love Don’t Need a Reason,” which he co-wrote with Peter Allen and Marsha Malamet. It still rings true today.
This is a cross-post from Karen’s LGBTQ+ Freedom Fighters Substack.
AIDS and HIV
AIDS Healthcare Foundation announces 3 million people globally in its care
Los Angeles-based group lauded ‘historic milestone’

The AIDS Healthcare Foundation, a Los Angeles-based nonprofit group founded in 1987 that has become the world’s largest HIV/AIDS organization, has announced it has three million people in care around the world.
In a statement released on May 26, the organization, known worldwide as AHF, said the latest accomplishment reflects its global commitment to HIV prevention, care, and treatment. It says the accomplishment comes at a time when AHF marks the 25th anniversary of its first global programs launched in South Africa and Uganda in early 2001.
The statement says the three million people in care milestone also comes while the group approaches the 40th anniversary of its founding in 1987.
“Today, AHF provides lifesaving services in 50 countries across Africa, the Americas, Asia, and Europe, supporting millions of people living with HIV through a network of 1,056 global clinics, 79 healthcare centers in the U.S., 67 pharmacies, 96 wellness centers, 26 Out of the Closet thrift stores, outreach programs, and community partnerships,” the statement says.
“This accomplishment is far more than a number — it represents 3 million individuals whose lives have been touched by compassion, commitment, and the belief that healthcare is a human right,” Condessa M. Curley, the AHF board chair, said in a statement. “We extend our deepest gratitude to every member of the AHF team whose dedication made this milestone possible,” Curley said.
The AHF website notes the organization was founded in 1987 in Los Angeles as a network of hospices committed to “fighting for the living and caring for the dying” at a time when there was no effective treatment for HIV/AIDS. A statement on the website says since that time AHF has greatly expanded, converting its hospices into healthcare centers “and building a new paradigm for HIV care both in the United States and around the world.”
The statement adds, “Under the leadership of president and co-founder Michael Weinstein, AHF has grown from a group of friends dedicated to creating dignified hospice care to the largest AIDS organization in the world.” It says Weinstein “has been at the forefront of creating cutting-edge healthcare and advocacy programs and continues to drive the organization forward with the aim of saving more lives around the world.”
The statement announcing the milestone has also come at a time when more than 40 million people worldwide are living with HIV, “while hundreds of thousands continue to die annually from AIDS-related illnesses despite the availability of effective treatment.”
It says AHF’s response has included an expansion of its prevention and public health programs worldwide. In 2025 alone, according to the statement, AHF and its affiliated programs provided nearly five million free HIV tests globally and distributed more than 54 million free condoms, “underscoring the organization’s continued emphasis on both prevention and treatment.”
In D.C. AHF operates health care centers at 1701 K St., N.W., Ste. 400 [202-293-8680], 650 Pennsylvania Ave., S.E., Ste. 310 [202-350-5000], and 1647 Benning Road, N.E., Ste. 300 [202-350-5000].
AIDS and HIV
SB 1023 takes aim at the invisible insurance barriers to HIV prevention
While injectable PrEP represents a major leap forward in HIV prevention, outdated insurance systems are keeping it out of reach for the people who need it most.
Some bills pass through Sacramento with the kind of pizazz you’d likely expect from a Heidi Klum Halloween party, while others tip-toe it as quietly as a mouse. More often than not, it’s the latter that carries more weight. SB 1023, recently advanced by the Senate Appropriations Committee and authored by Senator John Laird, falls into this second category. On paper, it’s about insurance billing codes and reimbursement pathways for injectable PrEP. In real life, it’s about whether prevention is actually accessible, or just theoretically available if you know the right pharmacy, the right paperwork, and the right brand of patience.
Let’s put this one in real talk. Injectable PrEP is one of the most promising tools we have in regard to HIV prevention at the moment. It’s long-acting, clinically effective, and designed to reduce the hassle of daily adherence that comes with its pill-form predecessor. The issue SB 1023 is looking at is not medical but bureaucratic. Some health plans cover injectable PrEP, but then funnel it through pharmacy benefits that don’t actually work for outpatient clinics trying to actually administer it. The result is a kind of administrative purgatory. The medication is there, the science is too, the patients are eligible and ready to go, and yet access gets stuck in the pipelines of insurance systems that were never designed for prevention as care. It appears that, when it comes to real care, they simply don’t.
Now, more than ever, even with the oral daily PrEP that we all know, love, and pop, this matters because prevention only works when it is accessible to the public that needs it, policy documents aside. When talking about PrEP and HIV prevention, we fall into the formulaic thinking of pop a pill, reduce the risk, and avoid the worst. Period. But anyone who has actually lived inside this system knows it’s more complicated than that. Prevention is impacted by income, stigma, clinic hours, insurance literacy, access to pharmacy, and whether you feel comfortable enough in a medical setting to keep trying. It’s shaped by whether your provider understands queer health without making you feel like a statistic instead of a person.
And for LGBTQ+ communities (especially queer and trans folks, Black and Brown communities, and sex-working communities), “usable” is the whole game. At face value, this is a policy fix. Realistically, it’s the recognition that HIV prevention still doesn’t distribute itself evenly across populations or communities.
There’s also something psychologically significant that’s happening here. Prevention is an emotional issue just as much as it is a medical issue. When access is accessible and stigma-free, folks can actually plan their lives without constantly negotiating fear and apprehension along the way. When unaddressed, you get something else entirely. Anxiety dressed up as responsibility. That specific flavor of anxiety that says, “You should be doing more,” while quietly making it harder to get up, get out, and do anything worthwhile.
I‘d be hard-pressed to harp on this topic without speaking on my own experience. I take Descovy every day. Not out of simple mindless routine, but as a practice of self-care. Like brushing my teeth, except with a much heavier historical and cultural context behind it. Some days it feels empowering, while other days it feels more like a reminder that prevention in queer life has never at all been passive. It is something we actively maintain in a world that has not always been necessarily interested in maintaining us.
And occasionally (and I say this with no shame), I also use doxycycline as I see fit in the context of post-exposure prevention practices. That, too, is part of a much broader shift in how we think about HIV prevention. It is less about singular solutions and more about layered strategies that meet people where they actually are, not where public health PowerPoints imagine them to be.
But the most real part about all of this is that, even when you are doing everything “right,” there is still an underlying buzz of vigilance. The medical history doesn’t lie. The knowledge that access can always tighten, loosen, or straight up disappear depending on politics, funding, or the latest moral panic.
That’s why SB 1023 matters. More than injectable PrEP, it’s about whether the systems around HIV prevention are evolving toward coherence or continuing to rely on the assumption that individual folks will simply absorb the friction. For our queer community, this bill sits inside a larger tension. We are simultaneously in an era of unprecedented biomedical capability and persistent structural inequity. We can prevent HIV with remarkable effectiveness, yet still struggle to make prevention consistently available across all the places it needs to be.
This gap has consequences for both physical and mental health. Physically, inconsistent access means preventable infections still occur. This is not only because tools don’t exist but because systems don’t deliver them cleanly. Mentally, it produces a quieter, more chronic strain: the stress of managing prevention as a personal project rather than a collective guarantee. It’s the difference between “I am protected” and “I hope I’ve done enough.”
This particular difference lives in the body. It shows up as vigilance fatigue. As decision exhaustion. As the low-level cognitive load of always tracking when prescriptions need refilling, when appointments need scheduling, and when insurance requires prior authorization that no one warned you about until you were already at the pharmacy window. And for communities already navigating stigma in healthcare settings, that burden is not evenly distributed.
So what do we do with a bill like SB 1023? On an individual level, we continue to use the tools and resources available to us, and we talk about them without shame. We normalize prevention not as a moral achievement, but as routine care. We share information in ways that don’t assume everyone has equal access to providers who understand queer health without hesitation or bias. We check in on each other not just about risk, but about access: “Are you actually able to get what you were prescribed?” We also resist the idea that prevention should feel isolating. No one should have to individually solve what is fundamentally a systems problem.
On a macro level, SB 1023 is a reminder that policy details are not details at all, aside from the difference between access and obstruction. It points toward a far more reaching need for healthcare systems designed around continuity rather than fragmentation. Systems that don’t require patients and clinics to constantly translate between medical intention and insurance interpretation.
It also raises the bigger question: if we already know how to prevent HIV, what exactly are we waiting for to make prevention universally frictionless? The science is not lagging. The barrier is administrative will. And administrative will is, in its own way, a form of public health intervention.
If we get it right, prevention becomes quieter. Not invisible, but integrated. Something you don’t have to fight for every month. Something that doesn’t require you to constantly re-prove your eligibility for safety. If we get it wrong, we continue to rely on individuals absorbing the inefficiencies of systems that were never built with us in mind.
I don’t think this bill is the end of anything. But it is a signal, small, specific, and important, that the conversation is shifting from “Do we have the tools?” to “Why are the tools still so hard to reach?”
For those of us who live inside that gap between availability and access, that shift is not in the least bit abstract. It’s very real, very personal, and long overdue. But that’s just one very gay man’s opinion.
AIDS and HIV
Fearless in the face of financial cuts: Alex Garner on HIV advocacy in 2026
As HIV programs face devastating cuts worldwide, Alex Garner explains why visibility, pleasure, and resistance remain acts of survival

At a time when global HIV funding is being absolutely gutted, and anti-LGBTQ rhetoric is at the mic 24/7, Alex Garner has little to no interest in softening the truth. As a longtime activist and leader at Mpact Global, Garner speaks with the sense of urgency that can only come from lived experience and witnessing history threaten to repeat itself in real time. For Garner, these financial cuts are not some abstract policy debate or a budget footnote. They are, with no doubt, life-and-death decisions that disproportionately endanger our queer and migrant communities and everyone living with HIV around the world.
In our conversation with this beacon of hope, Garner reflects on surviving three decades with HIV, the groundbreaking changes in queer sexual health since the early years of the epidemic, and why today’s political climate needs bold voices rather than shy whispers. As fearless as he is deeply compassionate, Garner makes the case that modern HIV advocacy is about pleasure, dignity, visibility, and refusing to let queer lives be treated as expendable. just as much as it is about medical treatment. PREACH.
Around the world, we are seeing funding for HIV and AIDS programs slashed. What is the undeniable and very real impact of these cuts, especially for communities of color?
Funding numbers may seem like figures on a spreadsheet to some, but they represent real lives. Queer people have and will die. That’s it in the most basic terms. Around the globe, queer people are severely vulnerable and are already working hard to get resources to support the community. Migrants, people living with HIV, and gender diverse folks are going to bear the brunt of these cuts.
What makes right now such a critical turning point for global HIV advocacy?
The science of HIV has made incredible advancements. We have the tools to radically change this epidemic, but we are lacking the will from those in power. They simply don’t care enough about our lives to make an investment. It has been 45 years since the HIV epidemic, and Mpact and our partners are still fighting for basic resources. Each day, we must continue to demonstrate that our lives have value and meaning.
Testing and education are often the first to go when budgets cut. Why are those two areas so essential to maintaining much needed progress?
Education is fundamental to public health. 45 years into the epidemic, we know that when it comes to community education, unfortunately, we have to do it ourselves. Mpact has worked in collaboration with various partners and social media influencers around the globe to create health promotion materials and content because it is needed now more than ever. Working with the community to ensure that health education is understandable, relevant, and culturally appropriate is critical to effective education initiatives.
Mpact Global is choosing to expand at a time when many organizations are pulling back. What’s behind that decision?
The anti-LGBT movements are growing around the world, and they expect us to pull back, but we are stepping forward. We must demonstrate that we are not afraid, that we are not going anywhere, and that the lives of our queer community matter and are worth fighting for. We also have a responsibility to step up since there are many partners around the world in places like Senegal, Ghana, or Indonesia, who are unable to do so without immense risk. We have to use our power and voice for them and the very real issues they face.
As someone openly living with HIV, how does your own story impact the way that you approach this work?
I have been living with HIV for 30 years. I have been HIV-positive for more years than I was HIV-negative. It impacts every aspect of my life. It’s created resilience, resistance, and a drive to keep fighting. Stigma is not going to hold us back, and we have to approach our work with a sense of fearlessness and shamelessness. We can build a community for queer people living with HIV, as it can empower people living with HIV while at the same time allow negative people to witness that a community is possible and that living with HIV is not something to be scared of.
Since the start of the 2000s, how has the world of queer health advocacy changed and what has gone unchanged?
In the past 26 years, the world of HIV has drastically changed. We understand that with successful treatment, people living with HIV can achieve an undetectable viral load. The primary benefit of being undetectable is that you can live a long and normal life. The secondary benefit is that it is impossible to transmit HIV. PrEP is also more than 10 years old. Both these advancements have changed the quality of life of gay men and have changed our sex lives.
We’ve witnessed a mini-sexual revolution where more gay men are pursuing the sex they want. They have prioritized pleasure and are not living in fear and anxiety due to HIV. Our desire for pleasurable sex and for connections has not changed, but the world around us has. We have dating apps and social media, for good and for bad, and we have Doxy PEP. It’s one more thing to allow gay men to have sexuality that is centered on pleasure and sexual satisfaction and not eclipsed by fear and risk. While many gay men may not have experienced the 80s and 90s, we don’t want gay men to live in fear.
With political hostility and legislative attacks are on the rise, how are HIV prevention and care efforts affected?
During these hostile times, anything that is seen as promoting the sexuality of gay men is the first to get cut. We’ve had similar things happen around reproductive health and health for migrants. It’s all interconnected, and it’s from a familiar playbook. It requires resolve, creativity, and coalition building to endure these attacks.
With Mpact Global operating in 62 countries, what are the common threads you’re seeing across regions?
Over 60 countries still criminalize same sex sexual behavior. Meanwhile, governments seek to criminalize us because of our HIV status, gender expression, sex work, or migration status. Responding to laws, policies, and authoritarian leaders who criminalize us is a through line. We mobilize, and we strategize. And at the same time, we find and build community, and we continue to raise our voices and put forth a narrative that demonstrates our humanity and need for fundamental human rights.
What does effective HIV advocacy look like today, as opposed to 3 decades ago?
Education, access, and control over one’s body. That has not changed much, and those are things central to HIV, reproductive justice, and basic human rights.
For younger generations who didn’t live through the early years of the epidemic, how do you convey the relevance and gravity of the issue?
We lived through the dark and difficult times so that the next generations don’t have to. I never want gay men to have to live in fear, shame, and guilt. I want them to be able to pursue their sexuality with abandon, passion, and desire.
We need to show them that our lives matter, that we are continuing to fight for our health and our lives all around the world, and that they need to be a part of it. We’ve got to work together. I want them to embrace their sexuality and never take it for granted. To not feel ashamed about their sex but to explore, and grow, and find pleasure.
How does intersectionality impact the future of HIV advocacy?
Everything we do is political, and all parts of our lives intersect with a variety of issues. Recently, the Mpact the Besoton Sidoso Internacional or International HIV Kiss-In was a public activation on the border in Tijuana to demonstrate the sexuality of queer people living with HIV and to highlight the issues faced by migrants on both sides of the border in relation to health, HIV, and sexuality.
What role has resilience and adaptability played in the work that you do with Mpact?
Mpact’s 20 years are defined by resilience. We’ve had to continue to fight for health and human rights even amidst very challenging times. There have been successes, but it’s evident, now more than ever, that gains, like access to antiretroviral medication, must continue to be fought for as they are not guaranteed. And even things we expect to be guaranteed, such as human rights, continue to be at risk, so we must be nimble in our response and organizing.
Where do you see HIV and sexual health advocacy in the next decade?
We need to normalize sexual health as part of our culture. They are viruses and bacteria and nothing to be ashamed of. We need to integrate them into our overall wellness, just like we do with cold and flu season. That requires more than just traditional advocacy; it requires a cultural shift. Culture will change and policy will catch up, just like with marriage equality.
What innovations, whether political, medical, or communal, give you a taste of hope at our current moment?
Social media is still an underutilized resource, particularly by progressives. Seeing queer people all around the world leverage social media to speak openly, honestly, and unashamedly about who they are and what they experience can transform our world and our politics. When queer people openly express themselves amidst many risks, it’s always a source of hope and inspiration.
If you could speak directly to global leaders and those responsible for slashing budgets, what would you want them to understand about the work that you do?
They need to understand that real lives are at risk. But sadly, I think that does not move them. People are dying and suffering all over the world, and policymakers are doing nothing. If they can’t lead, respect, and advance human rights, then they are not leaders, and they need to give up power and let others do the work.
As Mpact Global celebrates 20 years, what legacy do you hope the next 20 years will build for the next generation?
Community building is central to the work we do. We want to be a force for good that strengthens queer community and works in collaboration to ensure people can freely express their sexuality and gender, have control over their bodies, and continue to fight for health and human rights. Community has always been the legacy for queer folks, and we are dedicated to continuing that part of our experience.
Follow all things MPact Global
AIDS and HIV
Congresswoman Maxine Waters introduces new resolution for National Black HIV/AIDS Awareness Day
H.Res.1039 supports more funding, resources and awareness for Black American communities, who are disproportionately impacted by HIV/AIDS.

Today is National Black HIV/AIDS Awareness Day. Advocates established this day of awareness on Feb. 7, 1999, and nearly 30 years later, Black communities in the U.S. continue to be disproportionately impacted by HIV.
On Wednesday, California Congresswoman Maxine Waters introduced H.Res.1039, a resolution that supports the goals of National Black HIV/AIDS Awareness Day and calls for a collective commitment to address disparities Black people with HIV face. Waters represents the state’s 43rd congressional district, a majority Black and Brown population comprising South L.A. cities like Hawthorne, Gardena, and Inglewood.
In the resolution, Waters urges state and local government officials, as well as their public health agencies, to acknowledge the importance of this awareness day and encourage their constituents to get tested for HIV. The resolution also requests that the Secretary of Health and Human Services prioritize distributing grant funding to minority-led, HIV organizations and community-based approaches to fighting HIV stigma, LGBTQ+ discrimination, and racism.
In 2023, young Black men accounted for 47% of new HIV diagnoses among youth, while young white men made up 3% of these diagnoses, according to a new Williams Institute report. Black women also have the highest HIV diagnosis rate among women, and Black community members overall represent 38% of new HIV diagnoses and 39% of people living with HIV in the U.S., despite being only 12% of the national population.
Beyond the disproportionate rates of infection and diagnosis amongst Black Americans, these communities also face greater difficulties in accessing the medical care needed to prevent and treat HIV. In the same year, white Americans were 7 times more likely to access Pre-exposure Prophylaxis (PrEP) compared to Black Americans, a data point that affirms racial and healthcare inequities Black people continue to face in the U.S.
“[This] is a day to commemorate the impact of HIV/AIDS on Black Americans and encourage continued efforts to reduce the incidence of HIV, eliminate health disparities, improve access to care and treatment, and show support for all those who are living with HIV/AIDS,” said Congresswoman Waters, in a press release.
Waters has been an advocate for people impacted by HIV/AIDS since the peak of the crisis in the 1980’s. In 1998, she worked to establish the Minority AIDS Initiative, which expanded national prevention and treatment efforts in support of minority communities, who remain disproportionately impacted by HIV. In 2025, Waters introduced the “HIV Prevention Now Act” as well as the “PrEP and PEP are Prevention Act,” to increase prevention efforts and reduce health insurance barriers to access preventative resources, respectively.
H.Res.1039 is the latest addition to the congresswoman’s efforts to raise awareness for Black and other minority communities impacted by HIV/AIDS, and to fund and support on-the-ground efforts that prioritize their care and wellbeing.
The resolution is endorsed by various LGBTQ+ organizations mobilizing for communities impacted by HIV, including AMAAD Institute (Arming Minorities Against Addiction and Disease), LA Pride, AIDS Foundation Chicago, and PFLAG National. The resolution is also co-sponsored by 29 other U.S. representatives, including fellow California congressmembers Robert Garcia, Laura Friedman, Nanette Barragán, Sydney Kamlager-Dove, Lateefah Simon and Mark Takano.
H.Res. 1039 has been referred to the House Committee on Energy and Commerce, and currently awaits further action.
Kristie Song is a California Local News Fellow placed with the Los Angeles Blade. The California Local News Fellowship is a state-funded initiative to support and strengthen local news reporting. Learn more about it at fellowships.journalism.berkeley.edu/cafellows.
AIDS and HIV
From ACT UP to apps: A candid conversation with MISTR founder Tristan Schukraft
As HIV prevention ushers in a new era, Schukraft reflects on the evolution of sexual healthcare and the power of stigma-free prevention

It was not too long ago that an HIV diagnosis was read as a death sentence. In its earlier decades, the HIV/AIDS crisis was synonymous with fear and loss, steeped in stigma. Over recent years, open conversation and science have come together to combat this stigma while proactively paving the way for life-saving treatments and preventive measures like PrEP. Now, in 2026, with discreet and modern platforms that meet people where they’re at in their lives, HIV prevention has evolved from hushed words of warning into something far more sex-positive and accessible. Game-changing services like MISTR are a testament to this shift, showing our community that healthcare doesn’t have to feel clinical or shaming to work. It can be empowering and, dare I say, celebratory.
Few people embody this evolution quite like Tristan Schukraft, founder of MISTR. With one hand in healthcare and the other high-fiving through queer nightlife, Schukraft gets that, from the bar to the bedroom and beyond, prevention happens in person and in real life. His approach has helped turn PrEP, DoxyPEP, and testing into normalized parts of our daily queer life, reaching hundreds of thousands of people across the US.
In our conversation, Schukraft shares candidly about stigma, policy, and why the future of sexual health depends on keeping it real.
You have one hand in healthcare and the other in nightlife and queer spaces. Can you share with us how these two spheres impact and inform each other? How do they impact and inform you?
Honestly, for me, they’ve never been separate. Nightlife and queer spaces are where people meet, date, hook up, fall in love, and make friends. That’s real life. Being in queer spaces all the time keeps me grounded and reminds me who we’re building MISTR for.
MISTR markets sexual health in a sex-positive, stigma-free fashion. Can you share with us how you measure the impact of this approach?
This year, we held the first-ever National PrEP Day. Dua Lipa performed, and Cardi B was there. After the event, Cardi B went on her Instagram live to encourage people to sign up for PrEP.
When you make sexual health stigma-free and sex positive, people talk about it. We see it in how people use the platform. When 700,000 people are willing to sign up, get tested, start PrEP, and add things like DoxyPEP, that tells us we’ve made it feel safe and normal instead of scary or awkward. And then we see it in the results. Since we expanded DoxyPEP, STI positivity among our patients dropped by half.
How have you seen the conversation of sexual health in our LGBTQ+ community change in mainstream culture in recent years?
Ten years ago, nobody was casually talking about PrEP, and if they did, it likely referenced one being a Truvada whore. Now it’s part of the culture. Popstars like Troye Sivan post pictures of their daily PrEP pill on social media. Cardi B goes on Instagram Live telling people to get on PrEP.
For many sexually active gay men, taking PrEP is simply part of the gay experience. For people in more remote areas, it might not be as talked about. Particularly in rural or more conservative places, MISTR can be a life-changing option. No awkward visits to the family doctor or the local pharmacy where everybody knows your business. It’s all done discreetly online and shipped straight to your door.
You have publicly argued that cuts to government HIV prevention funding are of high risk. Would you please elaborate for us on what those budget decisions mean on an individual level?
It means real people fall through the cracks. Someone doesn’t get tested. Someone waits too long to start PrEP. Someone finds out they’re HIV-positive later than they should have. Community clinics will be the hardest hit, especially those in underserved communities. The good news is that MISTR is ready to help people who might lose their access to care. All you need to do is sign up at mistr.com, and it’s totally free with or without insurance.
From your (and MISTR’s) perspective, how do these funding cuts threaten ongoing efforts to end the HIV epidemic?
For the first time, we have all the tools to end HIV. If everybody who is HIV negative is taking PrEP and everyone HIV+ is virally suppressed, we can end all new HIV transmissions in the United States. We have everything we need today. All we need is to get more people on PrEP. Cutting funding risks losing that momentum. Ending HIV requires scale and consistency. Every time funding gets cut, you lose momentum, trust, and infrastructure, and rebuilding that takes years.
HIV transmissions don’t pause because budgets change.
In our current climate of decreased federal investment, what role do you feel private healthcare and business should play in sexual health?
With reports that the current administration is considering cuts to HIV and prevention funding, we face a moment of reckoning. At the same time, some employers are seeking to exclude PrEP and HIV prevention from their coverage on religious freedom grounds. If these challenges succeed, and if federal funding is slashed, the consequences for public health will be devastating. But this is where the private sector must step up to fill the gap, bridge divides, and deliver results.
Businesses have the power and platform to normalize HIV prevention and drive measurable outcomes. At MISTR, we see firsthand what’s possible: since introducing DoxyPEP, STI positivity rates among our patients have been cut in half. But it’s not just about medication. It’s about messaging.
Our sex-positive, stigma-free marketing speaks directly to our community, making sexual health part of everyday life. No awkward doctor visits, no needles, no paperwork — just free online PrEP and STI testing, prescribed by real physicians and delivered to your door. That kind of impact could grow exponentially if more employers embraced this approach and made HIV prevention part of their employee wellness programs.
Employers, this is your call to action. Start by making sure your health plans cover PrEP and DoxyPEP. Partner with platforms like MISTR to give employees private, stigma-free access to care. Offer on-site testing. Talk openly about sexual health, not just during Pride, but every day of the year. This is not political — this is about protecting lives, strengthening communities, and building a healthier, more productive workforce. Because healthy employees aren’t just good for public health — they’re good for business.
When the private sector steps up, outcomes improve. And when businesses align with platforms like MISTR, scaling impact isn’t just possible — it’s happening.
Has MISTR experienced any direct effects from these recent shifts in public health funding?
MISTR’s unique model is totally free for patients with or without insurance, and we don’t cost the government or taxpayers a penny. We are scaling up our efforts to reach people who might be losing their access or care.
What would be your message to policymakers who are considering further cuts to HIV/AIDS programs?
During his first term, President Donald Trump committed unprecedented resources to the Ending the HIV Epidemic initiative here at home. Bipartisan support has shown what’s possible when bold leadership meets smart strategy. To policymakers: I urge you to reconsider any cuts to HIV prevention funding. This is not the time to pull back. It’s the time to push forward. Ending HIV is within reach — but only if government, private industry, and community organizations stand together.
What is one perhaps overlooked win from last year that impacted you on a personal level?
Seeing our STI positivity rate drop by half after expanding DoxyPEP.
Looking at the year ahead, what are MISTR’s most significant priorities for sexual health in 2026?
Expanding access, especially in the South and in communities that still get left out. Rolling out injectable PrEP. And just continuing to make sexual healthcare easier and more normal.
Is MISTR planning to integrate injectable PrEP into the mix?
Yes, absolutely. Long-acting PrEP is a game-changer, especially for people who struggle with daily pills. We’re rolling it out through a hybrid model: telehealth plus in-person injections in key LGBTQ+ neighborhoods.
As you just mentioned, MISTR reported cutting STI positivity rates in half through expanded DoxyPEP access last year (mad props). What do you think allowed you to accomplish this?
We made it easy, normalized it, and bundled it into care. No stigma, no hoops, no lectures. When you remove friction, people take care of themselves.
If you could eliminate from our collective consciousness one particular myth or stigma about sexual health, what would it be?
Sexual health should be talked about in the open, and we can have fun with it! I threw a party in October for National PrEP Day. How many parties have you been to celebrating sexual health? You should go to more.
What were the most significant obstacles or setbacks you saw some of your patients face in accessing PrEP and STI prevention services in the recent past?
Stigma, paperwork, insurance, provider judgment, and just navigating a system that was never designed for them.
Looking at the next chapter, what would you like to see MISTR accomplish next? And I have to ask, what’s next for you?
For MISTR: scale, injectables, and getting more HIV+ utilizing MISTR long-term HIV care. I started MISTR with the goal of ending HIV, so this year, next year, and as long as it takes, I want to make history and end HIV.
For me: staying close to the community, building things that matter, and making sure we never lose sight of the humans behind the metrics.
For more information, head to HeyMistr.com.
This article is part of LA Blade’s January health series.
AIDS and HIV
Community is the cure: AIDS Walk LA returns to fight HIV and funding cuts
AIDS Walk Los Angeles returns to West Hollywood on October 12 with the theme ‘Community Is the Cure,’ highlighting the vital role of unity, radical community action, and advocacy in the fight against HIV/AIDS, stigma, and government funding cuts

APLA Health, a nonprofit providing HIV care, prevention, and sexual health services, announced the return of AIDS Walk Los Angeles on Sunday, October 12, 2025, starting from West Hollywood Park. This year’s theme, “Community Is the Cure,” emphasizes the role of unity in advancing progress against HIV/AIDS and supporting those affected.
Walk day will feature a live performance from RuPaul’s Drag Race star Heidi N Closet, DJ sets, and community booths. Following the celebration, walkers will make their way through the streets of West Hollywood.
“This event was born out of urgency, and it’s just as relevant today,” said Craig E. Thompson, CEO of APLA Health. “We’ve made incredible progress in the fight against HIV, but that progress is under direct threat from funding cuts and political attacks. Now is the time to show that we won’t be silenced or set back.”
Since its inception forty years ago, AIDS Walk Los Angeles has grown into one of the largest HIV/AIDS fundraising events in the world, raising nearly $100 million. Proceeds fund APLA Health’s services, including HIV specialty care, sexual health services, food and nutrition support, and housing assistance.
“The HIV/AIDS epidemic has always shown us that progress happens when people come together, when patients, neighbors, families, activists, and health providers stand shoulder to shoulder. Today, with funding under attack and stigma resurfacing, unity is not optional. ‘Community Is the Cure’ is a reminder that science alone isn’t enough. We need collective willpower, advocacy, and solidarity to ensure everyone has access to the care and dignity they deserve,” Thompson said.
Cuts to Medicaid, the Ryan White Program, and prevention funding threaten access to medications, housing assistance, and food security. “Here in Los Angeles, where tens of thousands rely on these programs, even modest reductions can push people back into crisis. AIDS Walk Los Angeles helps fill some of those gaps, but philanthropy cannot fully replace the government’s responsibility,” Thompson explained.
Communities of color, the medically underserved, people living in poverty, and those experiencing homelessness are disproportionately affected. “The barriers aren’t medical. They’re structural: stigma, lack of insurance, unstable housing, and underfunded safety-net services. The administration is underinvesting in the very programs designed to break down these barriers. Until that changes, inequities in HIV prevention and care will persist,” he said.
Funds raised by the walk provide housing, groceries, case management, and access to medical care. Thompson shared the story of one patient who had lost housing and had to choose between medication and meals. “Through AIDS Walk–funded programs, we were able to connect him to stable housing, consistent medical care, and our food pantry. Today, he is virally suppressed, working again, and mentoring others who are newly diagnosed with HIV. Stories like his are common, and they remind us that cuts aren’t just numbers on a spreadsheet, they’re setbacks in real people’s lives.”
Beyond fundraising, AIDS Walk LA is a platform for advocacy. “When thousands of people flood the streets of West Hollywood, it’s a visible reminder to our community that HIV/AIDS has not gone away and to policymakers that their decisions have life-or-death consequences. The walk puts pressure on elected officials to fund programs, fight stigma, and stand up for people affected by HIV,” Thompson said.
He urged the public to take action beyond walking and donating. “Call your elected officials. Demand that HIV services remain fully funded. Show up for community hearings. Support housing initiatives. Share facts on social media to counter stigma. And, importantly, talk. Without continued conversation about HIV/AIDS and sexual health, we jeopardize the incredible advancements we’ve made in HIV care and prevention.”
Thompson also framed the walk as part of a broader activist approach. “Radical action today means showing up for one another in tangible ways, housing someone, feeding someone, advocating for someone, and refusing to accept policies that erase people’s humanity. As our theme emphasizes, when politicians fail us, COMMUNITY IS THE CURE. For participants in AIDS Walk LA, it means recognizing that the walk is just the beginning. Each person can be a messenger, an advocate, and an ally in daily life. When we work together to get people connected to support services, the collective action is radical because it insists on care and dignity in a time when those values are under attack.”
“Activism ensures policymakers cannot quietly dismantle programs. Community solidarity means that no one gets left behind. Public pressure creates accountability. When thousands unite at AIDS Walk LA, it demonstrates the broad mandate to keep fighting until HIV is no longer a public health crisis. That unity is as important as any medical breakthrough,” Thompson concluded.
For more information on AIDS Walk Los Angeles and how to register, visit https://AIDSWALK.LA.
AIDS and HIV
“If not now, when?” Journalist and activist Karl Schmid is reshaping how we talk about HIV/AIDS
The Blade sits down with the award-winning host to talk about stigma and his latest initiative – taking HIV education onto the runway

Karl Schmid has long been a staple in queer news and media. Hailing from Australia, Schmid grew accustomed to the limelight from a young age, and eventually made a successful transition into American network television through his work on red carpets for ABC.
In 2018, he would be thrust into the spotlight for a different reason. Despite repeated warnings from professional acquaintances, Schmid came out as HIV positive to share his story, wear down stigmas, and to educate people about important and misunderstood science like the concept of undetectable equals untransmittable.
And so, Schmid would grow accustomed to renewal. In 2019, he launched Plus Life Media, a platform that shares HIV resources, education, and stories of resilience from people living with HIV/AIDS. He was part of the team behind the Emmy-nominated short documentary, Marty’s Place: Where Hope Lives: an intimate look into a housing cooperative created in the 1990s to support people with HIV/AIDS. Late last week, he flew to New York for the U.S. debut of his latest initiative: HIV Unwrapped. The project pairs researchers and scientists in HIV studies with fashion design students, culminating in a runway show that features bold reimaginings and interpretations of crucial science.
The Blade spoke with Karl about the cross-pollination in his own life and career, and how his latest effort is shaping the way he blends activism and media to reinvigorate conversations around HIV/AIDS.
HIV Unwrapped feels like a really interesting pivot into a different kind of modality and platform for you. Can you tell me more about the initiative and how it fits into your legacy of activism and work?
Well, HIV Unwrapped came out of Australia and this wonderful activist named Brent Allan, who I’m good friends with. And Brent had been at, I think, the WorldPride, or something that was happening in Australia, and there was an exhibition where they paired some engineers and science people of varying professions with a fashion designer to try and illustrate their work.
And he thought, “Wow, what a great way to maybe try and interpret HIV science and reignite the conversation around HIV.” So it started in Melbourne, Australia, and it was successful there. And then they did a version in the UK earlier this year. And then in July for the International AIDS Conference that took place in Kigali, in Rwanda, they did a version.
And that’s kind of where I stepped in. I think with HIV Unwrapped, you’re drawn into the fashion first — and then the science comes. It’s just a really unique and different way of reframing the conversation about HIV. But beyond that, it’s also working with fashion students, young people, and to see them become so invested in HIV science. That’s what gets me the most excited. Because you’re opening a whole new world to a person who doesn’t maybe really think about HIV all that much, and now they’ve learned all this amazing stuff. Suddenly you’ve got a whole new bunch of people talking about HIV in exciting and fresh ways, and they’re telling their friends and they’re having conversations about it.
You’re trying to create different entry points for people to not only talk about the science behind HIV and AIDS, but also how we can reinterpret it in original and visually interesting ways.
I mean, look, you’ve got the House Appropriations Committee willing to advance this “Big Beautiful Bill” that slashes $2 billion in HIV funding in this country, and as someone living with HIV, you keep going, “Why would they do that? Why? We are so close to ending HIV.” All of a sudden, we’ve stopped funding research, and we’re stopping this, and I’m just like, “Why?”
Now more than ever, we’ve got people and politicians and government and a large part of the United States who think, “Oh yeah, HIV isn’t a thing anymore. It’s not important.” Well, it is still a thing. It is still important, and HIV Unwrapped is a way to be creative and open new avenues of dialogue.
A friend of mine sent me a handwritten note the other day. This is in Texas. One of his roommates wrote a handwritten note to another roommate, saying, “Oh, just so you know, ‘such and such’ has AIDS. So I’d be scrubbing the shower if I were you after he uses it. I personally have decided to go and shower at the gym.” And this is a person in their 30s, so we’re still having these dumb conversations from 1984.
That’s why I do what I do with Plus Life, and that’s why I’m like, “Wow, HIV Unwrapped is another tool in our toolbox we can use.” And I guess our hope is really that scientists will see this across the country and around the world and go, “Well, that is a really cool way to explain my science and make it accessible,” and want to engage in future projects like this.
How queer communities are represented in the media can leave deep imprints. I was watching an older interview you did where you recall this HIV ad you saw in a movie theater as a kid. The Grim Reaper’s there, and it’s creepy and sinister. It seems like we’ve moved away from that kind of imagery — but it doesn’t feel like we’ve necessarily come to a much better understanding of HIV/AIDS. Where do you think we’re at now in terms of representation?
The fact that, to this day, I can tell you where I was, what the movie was, that it was a Saturday, which cinema it was in, and I was a seven year old kid. It gives you an idea of how burned into my memory that is. And, I agree. I think we’ve moved away largely from the fear tactics, but we’ve stopped talking about it. I’d like to think that we’ve gotten better in representing people living with HIV, on television and film, as just people living with HIV. Where HIV doesn’t become the central storyline, and it’s not a doom and gloom, “woe is me” story. It’s just part of who they are.
But we sort of dance around anything that’s to do with our bodies or sex or sexuality, because it makes us uncomfortable. And so when I pitch stories to ABC and other networks, and even, quite frankly, trying to get press to cover HIV Unwrapped: we get passed on. People don’t want to talk to us because HIV isn’t sexy. As long as we keep doing that and having that reaction — if we don’t talk about it — we don’t get to a place where we can be comfortable with it.
Since I came out about my status all those years ago, my focus has been trying to normalize the conversation. That’s how we grow, and that’s how we learn — whether it’s HIV, whether it’s politics, whether it’s anything. But if we don’t talk about it, and we sort of pretend it doesn’t exist, and then we cut funding for it, and we sort of sweep it under the rug: it ain’t going to go anywhere.
Women of color, Black and brown women, have the highest infection rates in the United States. In the south those rates keep going up and up and up, and now we’re cutting funding to testing and to counseling and to services. I’m really worried that we will end up back with AIDS wards in hospitals again, and there’s no need for it.
To bring it back to HIV Unwrapped, that’s why, if I can come up and work with an amazing group of people to tell stories and to have conversations in fresh ways, then I’m going to keep doing it — whether it’s HIV Unwrapped, whether it’s what I do on Plus Life, whether it’s a television show or whatever crazy thing I come up with next.
It feels like there’s so much watering-down in terms of conversations around sexual health, HIV and AIDS. What is the resistance that you’ve faced, and how has that resistance changed over the years?
I’ve heard, “I think what you’re doing is great. It’s just not the right time to tell the story.” Well, when is the right time to tell the story? I think so many people in America think HIV doesn’t affect them. And the reality is very different. HIV affects everybody. If not now, when? People are still dying in this country. People are afraid to get tested, and they’re living in shame. And they’re hiding what’s wrong with them because of the stigma — and that just shouldn’t be happening.
I’ve said this a million times too. You know, HIV and AIDS doesn’t kill you. That’s not what’s going to put me in the grave. But it’s the stigma. It’s the bigoted, out-of-date opinions of Congress and politicians and public figures and uneducated people who just think this is somehow some deviant, dirty “sex disease” or drug disease, and those of us who get it deserve it. And you know, television networks, especially, are in the business of making money. And to do that, they sell advertising, and so they’re worried that advertisers will turn off if you talk about this kind of stuff.
And I think it’s maybe a little bit the opposite. I think if you can find, again, engaging and interesting ways to have real conversations, I’ve certainly found that you get a very vast and wide audience of people who will chime in and may have an opinion. And again, our opinions may differ, and that’s okay, but, but as long as we’re having the conversation, the more you say it, the less scary it is.
Almost 20 years after you were first diagnosed with HIV, do you see yourself pivoting now to work more on activism? Is that something you’re trying to focus more on now at this point of your career?
I will say that I’m incredibly fortunate to have worked for as many years as I have in broadcast, and I’ve done some really amazing things, and had some phenomenal opportunities going to the Oscars and doing all those red carpets and celebrity interviews all over the world. They’re all valuable experiences that I’ve been able to build upon. But I will say that in the last sort of two years, especially, my focus has become more about Plus Life and doing these kinds of stories and these kinds of initiatives.
I am fascinated by people. I think to be a decent journalist or broadcaster, you have to have that innate curiosity. And I am deeply curious about people and people’s behavior and where they come from, and what kind of homes they grew up in, what their friends are like. It’s incredibly satisfying to me. Do I miss being on regular, scheduled programming and television? Sure. It was a fantastic platform, and there’s nothing quite like the thrill of live television for me, and that’s why I loved being in news and entertainment news.
I think as I sort of get older, and I’m no longer the young kid on the block, and I’m not so nimble with my thumbs and my forefingers when it comes to putting stuff up on social media and Tik Tok and all of that…If I’ve got an opportunity to really hone in on the stuff that I do with Plus Life, there’s nothing more rewarding than that, right?
A behind-the-scenes documentary of the U.S. debut of HIV Unwrapped will be available to stream on November 30th, just before World AIDS Day.

Aging with HIV: The Latino Commission on AIDS honors National Latino Older Adults & HIV/AIDS Awareness Day

Here’s Your Palm Springs Weekend: Jul 24-26, 2026 by LA Blade x Gay Desert Guide

At Alliance Defending Freedom’s summit, church and state are one

OutfestNEXT shows us the true power of queer cinema

2026 International AIDS Conference to take place in Rio

DOJ seeks to dismiss some claims in gay FBI employee’s bias lawsuit

Black, gay Elijah Manley is running against Florida stalwart Debbie Wasserman Schultz for Congress

Sci-fi has long been at vanguard of LGBTQ+ representation

In the middle of the Bible Belt, a summer camp lets trans kids exhale

The LA Blade Take: ‘Stop! That! Train!’ is a camp, queer, high-speed RuPaul vehicle with some misses, now available on streaming
-
 National4 days ago
National4 days agoDOJ seeks to dismiss some claims in gay FBI employee’s bias lawsuit
-
 Politics2 days ago
Politics2 days agoBlack, gay Elijah Manley is running against Florida stalwart Debbie Wasserman Schultz for Congress
-
 Arts & Entertainment4 days ago
Arts & Entertainment4 days agoSci-fi has long been at vanguard of LGBTQ+ representation
-
 North Carolina3 days ago
North Carolina3 days agoIn the middle of the Bible Belt, a summer camp lets trans kids exhale
-
 Movies2 days ago
Movies2 days agoThe LA Blade Take: ‘Stop! That! Train!’ is a camp, queer, high-speed RuPaul vehicle with some misses, now available on streaming
-

 Puerto Rico3 days ago
Puerto Rico3 days agoLGBTQ+ ‘human rights crisis is unfolding in Puerto Rico’
-
 Brazil1 day ago
Brazil1 day ago2026 International AIDS Conference to take place in Rio
-

 Poland3 days ago
Poland3 days agoPolish president vetoes same-sex relationship recognition bills
-

 National2 days ago
National2 days agoRemembering Victoria Cruz, Stonewall veteran and beloved trans activist
-
 a&e features24 hours ago
a&e features24 hours agoOutfestNEXT shows us the true power of queer cinema