
Health
Dr. Rachel Levine speaks with trans youth at D.C. health clinic
Youth Pride Clinic is one of the few clinics in the nation to provide primary care & mental health services to LGBTQ youth from ages 12 to 22

WASHINGTON – It’s not unusual for Rachel Levine as assistant secretary of health to visit medical facilities on behalf of the Department of Health & Human Services. But her visit last week to the LGBTQ youth clinic at the Children’s National Medical Center was special because she was able to meet with transgender youth as an openly transgender presidential appointee.
The visit on Thursday by Levine at the D.C.-based hospital comes not long after the U.S. Senate approved her appointment, making her the first openly transgender presidential appointee to win a Senate-confirmed position. As such, her visit to the LGBTQ youth clinic, where transgender kids come for transition-related care and health services, held particular significance for the patients.
Levine, speaking with the Washington Blade at the end of her visit, said having the opportunity to speak with both transgender youth and medical professionals testing them was “tremendously, tremendously rewarding”
“It’s tremendously gratifying to be able to speak to the medical professionals and the clinic personnel at beds, particularly to the youth and their families from my experience,” Levine added. “So I have two aspects of that. One is that I’m a pediatrician and adolescent medicine specialist. So I’ve been teaching to children and their families my entire career, but the other is coming from my lived experience as an openly transgender woman, and so I find it tremendously rewarding.”
The warm environment of the hospital for children is readily apparent upon entering the main atrium of the building. Lights dressed up as hot air balloons fill the tall ceiling while a nearby TV shows music videos consisting of squares of kids’ faces singing, followed by easy-listening country music and Asian K-pop. Children and their parents await their appointments seated in comfy plush red chairs before white blocks meant for use as tables.
Key to Levine’s visit was taking part in a discussion at the hospital auditorium with three transgender youth and their families who obtain services at the clinic. During the question-and-answer period, Levine shared her experience as a transgender person who underwent transition later in life and went on to tremendous success as a high-ranking presidential appointee.
For the transgender youth, Levine’s presence at the hospital — at a time when state legislatures are busy enacting bills to restrict their access to medical care and school activities — serves as a reminder that barriers based on gender identity are breaking down and the sky’s the limit for their future.
After the question-and-answer session, Levine told the Blade she “learned a lot” about the Children’s National Medical Center, which she called “a world-renowned children’s hospital and academic medical center.”
“I’ve known about it before,” Levine added. “I’m a pediatrician, adolescent medicine specialist, but I learned more about what they’re doing. And I learned specifically about their gender clinic, where they take care of transgender and gender non-conforming youth and got to meet some of the staff as well as the kids and their families.”
The Youth Pride Clinic, which opened in 2015, is one of the few clinics in the nation to provide primary care and mental health services to LGBTQ youth from ages 12 to 22. Among the services offered are hormone replacement therapy, STP/STI treatment and PrEP services as well as individual and family therapy for transgender youth.
Among the transgender youth patients at the clinic who spoke to the Washington Blade was Amir, a 15-year-old Georgia native whose last name as a minor is being withheld for confidentiality purposes.
“I started out in fifth grade coming out as lesbian,” Amir said. “I didn’t even really know, but when I came out to my grandma in Georgia, where I’m from, I still didn’t feel like myself. So then, later on, me and my friend researched, and next thing you know we came across the term transgender, and I was like, ‘This is who I am. This is me.’”
Amir said he began taking shots as part of care regimen in January. Being able to receive care from the Youth Pride Clinic, Amir said, means a lot because he has an opportunity not available to other transgender youths, who face challenges and even hostility as they make the journey to transition. The staffers at the Youth Pride Clinic, Amir said, are “like a second family” who work hard to provide the services they offer.
Sonia Murphy, Amir’s aunt who became his legal guardian, said when she began reaching out for medical help for Amir she found a two- or three-year wait list to get access to treatment, which she said makes her “saddened” such care isn’t widely available.
“There’s a population of kids and parents out there who need the services and just can’t access it because there’s not enough bandwidth, not enough manpower,” Murphy said.
Amir said he’s getting other avenues of support from his two cousins, one who is older at age 18 and one who is younger at age 12. “They’re like sisters to me, so I call them my sisters,” Amir said. Amir also identified two other male cousins as well as his uncles and his aunt.
“They’re all very supportive of me,” Amir said. “My auntie Tonya, for example, Pride month came up, first day, she sent me a paragraph, saying, ‘I’m glad you’re yourself and you’re open to who you are and things like that,” and that I’m not afraid to be who I am around anybody. It’s just things like that. And for my birthday, I had tons of Pride shirts, and I got a rainbow shirt with the fist in the middle for Black Lives Matter, and it was a ton of different things.”
Lawrence D’Angelo, director of the Youth Pride Clinic and an occupational health adolescent medicine specialist, told the Blade being able to start the facility in 2015 in and of itself was one of the key victories for the initiative, although he said the Children’s National Medical Center has been providing transition-related care since 1998.
“When we started it…we thought that we were going to be running a PrEP clinic, that we were going to be providing preventive services to LGBTQ kids,” D’Angelo said. “The first day, the first patient actually came in and asked for PrEP, and the other six patients that were scheduled that day all wanted transgender services. So, suddenly, it became obvious what we were going to be spending 90 percent of our time doing, which is exactly what we think we should be doing, because that’s where the need is the greatest.”
Despite the advantages of having access to the Youth Pride Clinic, transgender youth have clear challenges and face hostility based simply on their gender identity, especially in a year when state legislatures have in an unprecedented manner enacted legislation against them. The Youth Pride Clinic, in many ways, is an oasis of support.
Arkansas, for example, enacted a measure that would make criminal the kind of services provided at the clinic. Other states have enacted measures prohibiting “biological boys” from participating in sports, which essentially bars transgender girls from participating in sporting events.
While anti-trans measures aren’t being enacted in D.C. or any nearby states, the advancement of anti-trans legislation in states has had a negative effect on transgender patients at the Youth Pride Clinic.
D’Angelo, based on conversations he’s had with the patients, said they’re aware of the wave of legislation, which he said has led to fear, anger and being “unable to understand what is happening and why it’s happening.”
Amir said watching states enact legislation against transgender youth “makes me feel some type of weight,” pointing specifically to the anti-trans sports measures because he said he’d welcome the opportunity to participate in athletics.
“I’m athletic,” Amir said. “I do all types of sports. I play basketball, soccer, I’m going to do boxing…With sports and stuff, I just feel like I want to be able to do everything, just as a regular cisgender person will be able to do,”
Amir, despite the enactment of anti-trans laws, has an optimistic outlook and said the enactment of state measures against transgender youth demonstrates they’re now “on the radar” of the social conservative movement.
“I feel like if everybody who’s a part of LGBTQ and trans together, we can stand up and we can overcome this because the thing is, there are so many people out there who don’t understand what we do, and the thing is that they’re noticing us, so that’s a start to something big.”

With many states hostile to transgender youth, others are looking to the federal government for support under the Biden administration. On his first day in office, Biden signed an executive order directing federal agencies to implement the U.S. Supreme Court’s decision against anti-LGBTQ discrimination to the fullest extent possible.
Levine cited an announcement from HHS that resulted from this order on implementing regulations prohibiting anti-LGBTQ discrimination in medical care, reversing a policy under the Trump administration that green lighted discrimination, as one of the ways it has answered that call and helped families like the Youth Pride Clinic.
“So the Affordable Care Act says that you cannot discriminate based upon sex,” Levine said. “The Department Health & Human Services and the Office of Civil Rights has interpreted sex to include sexual and gender minorities, to include sexual orientation and gender identity, which means LGBTQ individuals under that. So we need to look at all aspects of the Affordable Care Act, and to work to implement that interpretation of the statute. That was only done a month or so ago, so we’re going to be working on that now.”
Is there anything more the federal government can do to support the clinic? D’Angelo cited a number of key things already secured, including the hospital being able to offer insurance to patients and the affirmation from HHS against anti-LGBTQ discrimination. More research dollars and greater focus from the National Institutes of Health on gender diverse and sexual minority individuals, D’Angelo said, would also be welcome.
“There are things out there that the federal government can do, but I think…there are limitations of what they can do,” D’Angelo said. “They can’t, unfortunately, effect what’s going on in individual states, which is, in some cases draconian. That’s an awful thought if we were practicing medicine in Arkansas, we could be in jail.”
Meanwhile, Levine said the Biden administration, including Secretary of Health & Human Services Xavier Becerra, is working on both internal and external policies to facilities like the Youth Pride Clinic to help them secure their place in the health system and reach transgender youth.
“The secretary and I will be doing everything we can to advocate for the LGBTQ community,” Levine said. “So I think we’re going to be working externally, in terms of advocacy, and then we’re going to be working internally in terms of policy.”



Commentary
Breaking the mental health mold with Ketamine: insights from creator of Better U
How this brand is making high-impact mental health care available to the people who need it most

Ketamine therapy was once on the fringe, but now makes up a fast-growing field in the world of Mental Health. Derek Du Chesne of Better U, a mental health service in West Hollywood, shares how his team attempts to make psychedelic care safer, smarter and more accessible.
Mental health is finally getting the attention it deserves and as our understanding of it deepens, so does the range of tools available to support it. In recent years, psychedelic-assisted treatments like ketamine are gaining serious ground and a growing number of clinicians have turned to these as promising alternatives to more traditional methods. Enter Du Chesne, creator of Better U, with the goal of making ketamine therapy more accessible and personal. In our conversation, Du Chesne shares the mission behind Better U, the challenges faced by underserved communities and how his team is aiming to reshape the mental health landscape one patient at a time.
Can you share what Better U is all about?
I’m the founder and CEO of Better U. We’re a telemedicine-based alternative wellness platform, currently operating in 35 states. We primarily offer ketamine therapy for conditions like depression, anxiety, PTSD and suicidal ideation. We also provide services in sexual health, clinical weight loss and holistic psychiatry.
You’ve had your own experience with psychedelic therapy. Can you talk about how that journey inspired Better U?
Six years ago, I never imagined I’d be doing this. I had used psychedelics recreationally, but ketamine never interested me. I saw it as a horse tranquilizer nothing I’d ever take seriously.
I had been working in alternative health, specifically cannabinoids mainly on the supply chain side across several industries. In 2019, I traveled to about 40 countries for work and we raised around $40 million in capital. That year, my company made $85 million in revenue and was heading into a $1.2 billion acquisition. Personally, I was also about to get married. Within six weeks, both my career and my relationship unraveled. The company let me go just before my equity vested and I later found out my fiancée had been unfaithful while I was on the road.
Everything I had built my identity around collapsed. I spiraled into a deep depression, tried therapy, psychiatry, and antidepressants. None of it helped. Eventually, I became suicidal. A close friend intervened and brought me to a ketamine clinic. I was extremely skeptical, especially since a single session cost $1,600. But about 15 minutes into it, I felt like I could breathe again for the first time in months.
The treatment helped me separate from the constant, negative thought loops. It created space between me and my pain, helping me see that the things that happened didn’t define me. That clarity changed everything. I no longer felt like I had to carry shame or blame for what others had done. It gave me peace.
Shortly after, a friend suggested I get out of my environment. Everything in my home reminded me of the past. I went to The Bahamas for a reset: sun, exercise and healing. That period helped me recalibrate.
Months later, I was invited to Stanford by a friend whose sister leads epidemiology there. At dinner, I met someone involved in psychedelic research. I shared my experience and he invited me to visit their depression clinic and psychedelic research lab. That’s when I realized the transformative potential of these therapies. I sat with hospice patients receiving psychedelic treatments. People from all walks of life have similar, profound responses. It was incredibly moving.
That’s when I started thinking: how do we make this affordable and accessible? My first ketamine session was powerful, but afterward, there was no follow-up, just a “see you next week.” It felt transactional. I wanted to build something more thoughtful, especially for people like those in my small hometown in Wisconsin where mental health care is rare and stigma is high.
Better U was born from that idea.
Better U has facilitated over 230,000 sessions for around 18,000 patients nationwide. A large portion of your clients identify as LGBTQ. Why do you think ketamine therapy resonates so deeply with that community?
The LGBTQ community is incredibly diverse, and so are the challenges its members face, from gender dysphoria and identity struggles to rejection from family, friends, or society. That rejection often comes right at the moment someone begins living as their authentic self. The emotional toll can be devastating and in many cases, the suicide rates, especially among trans individuals, are alarmingly high.
Ketamine therapy creates space. It allows someone to step outside of the emotional chaos, the shame, fear, judgment and look at themselves without that mental noise. When you can separate your identity from the voices in your head or the reactions of others, there’s clarity. You begin to realize, “This pain isn’t about who I am, it’s about others’ inability to accept me.” That shift can be life-saving.
Many of our LGBTQ clients come to us after years of self-medicating with alcohol, drugs, or even unhealthy relationships. Others feel like they’ve hit a wall with traditional talk therapy. As we age, our brains get more set in their patterns. Ketamine disrupts those patterns. It can help people access a deeper level of understanding and healing, especially when other methods have stalled.
What’s powerful is that many patients don’t come in intending to stop drinking or using substances. They come for anxiety, depression, or suicidal thoughts. But after a few sessions, they’ll say, “I realize my drinking is tied to social anxiety,” or “I use because I feel like I have to numb myself to be accepted.” The therapy helps them see that those coping mechanisms aren’t serving them anymore.
We’re based in West Hollywood, so we’re deeply embedded in this community. In cases of suicide attempts, local hospitals like Cedars-Sinai often reach out to us because ketamine has become one of the most effective tools for treating suicidal ideation.
That said, it’s not a cure-all. If someone is abusing ketamine recreationally, we won’t treat them with it. It’s not safe or appropriate. But in a clinical setting, when properly dosed and supported with integration care, we’ve seen almost no cases of addiction. It can be a powerful tool for healing when used with intention.
Trauma-informed care is a term that gets used a lot in mental health these days, but what does it actually mean to you and how do you apply that framework at Better U?
To me, trauma-informed care means creating a system where every person interacting with a patient, from intake to integration, is trained to recognize, respect and respond to trauma. At Better U, we’ve built multiple layers of support to reflect that. While our welcome team handles basic screenings and eligibility, it’s our clinicians, integration therapists and success team who are most deeply trained in trauma-informed practices.
The unfortunate reality is that many ketamine clinics are founded by anesthesiologists—people who understand how to use the drug medically, but have little or no training in mental health. You can see it when you look at their teams: no psychotherapists, no psychiatrists, no trauma-informed staff. That’s dangerous, especially with a treatment that has the potential to surface deeply emotional material.
At Better U, we made sure to embed trauma-informed care into our clinical culture. Our doctors like Dr. Zaa Faul—a dual-board-certified addiction specialist and Army veteran—and Dr. Jamie Brooks, have deep expertise in both mental and physical health. Our success team, which supports patients after their sessions, is mostly made up of licensed therapists and professionals with years of experience in crisis care, psychedelic research and emotional integration.
Trauma-informed care also means learning how to hold space for people in distress. When I was the only person speaking to patients in our early days, I got yelled at, cussed out, blamed, not because patients were “bad” people, but because they were in pain. Maybe they hadn’t slept, or fasted before a session and were feeling raw. Maybe they were grieving or reliving trauma. You have to meet people where they are, understand that it’s not personal, and guide them toward healing without judgment. That’s where nonviolent communication becomes essential too. It’s a big part of how we train our staff.
Ultimately, it’s not just about delivering a treatment. It’s about helping people feel seen and safe enough to transform. And when you do that well, you get to witness incredible things, like someone processing deep grief or suicidal thoughts in a matter of weeks, instead of years. That’s the beauty of this work.
Let’s say I’m a potential patient who’s hesitant of undergoing ketamine therapy. What would you say to ease my mind?
Sure. First, I’d ask, have you ever had any experience with psychedelics?
[Then, I’d explain] most people who come to Better U, probably over 95%, have never had any experience with psychedelics. So it’s completely normal to feel anxious going into a first session and entering an altered state of consciousness. Especially if it’s unfamiliar.
I want to be transparent—our program isn’t a microdose. It’s a full, immersive experience.
That said, let me walk you through what the process actually looks like so you know what to expect.
After a consultation with a doctor to make sure this is a safe and appropriate treatment for you, you’ll receive a kit in the mail. That includes a blood pressure cuff, a journal, a “brain box,” and other tools to support your experience.
Then, before your first session, you’ll have a mandatory preparation meeting with one of our therapists. That’s where you can ask any remaining questions or talk through any lingering anxiety. You can even request a group session if you want to hear what others are feeling.
We also start very slowly. Your first dose is intentionally low — it won’t feel like a full psychedelic trip. It’ll feel more like a medication-enhanced meditation. It’s really just a way to help you dip your toe in and see how your body and mind respond before we increase the dose.
Is it safe?
Yes, incredibly safe, when done properly. Our protocols are built to prioritize your safety at every step. We’ve worked with thousands of patients and have seen incredibly low rates of any negative outcomes, especially when compared to traditional psychiatric medications.
And to be direct, while this work can be uncomfortable at times, it’s not always sunshine and rainbows, it’s also where the breakthroughs happen. This treatment acts like a mirror, helping you see what’s going on inside, but from a different, often clearer, perspective. And sometimes just that shift in perspective can change everything, from how you relate to yourself to how you engage with the world around you.
Where do you see Better U going in the near future, and how do you see it shaping the future of mental health?
Right now, one of our primary focuses is on insurance credentialing for all of our providers. Most of our patients come to us already on medications – antidepressants, benzodiazepines, Adderall, and so on—and as things currently stand, we can’t legally give them a plan to taper off or discontinue those medications.
So, let’s say someone goes through eight ketamine sessions with us and feels amazing, but they’re still on Xanax or an SSRI—we can’t formally help them get off of it. I think a huge issue in the U.S. right now is over-diagnosis and over-prescription. So by getting our doctors credentialed to accept insurance, including Medicare and Medicaid, we can create six month plans.
For example, to help patients reduce or discontinue medications that may no longer be serving them. At the very least, we want to help people lower their dosages to give themselves a fighting chance. Because right now, mental health care in this country is incredibly broken.
We’re also implementing AI. We’re about to launch a 24/7 companion app that provides continuous support. I think one of the reasons Alcoholics Anonymous has been so successful is the sponsor model. We’re building something similar: an AI “sponsor” or companion that can provide round-the-clock mental health and physical wellness support. Think of it as an AI therapist that works alongside the human element.
Looking further ahead, we’re also preparing for the future of MDMA-assisted therapy, psilocybin and other emerging treatments. There’s a lot coming and we’re positioning Better U to be at the forefront of it all.
Viewpoint
I’m a queer Iranian Jew. Why I stand with Israel during this conflict
‘Hands Off Iran’ movement is erasure, not solidarity

The sirens cut through the night, jolting me from sleep. My heart pounds as I lie in bed, listening to the explosions outside. I don’t have to run — my Airbnb bedroom is a “mamad,” a reinforced bomb shelter built into the apartment. Though the windows are sealed, I can feel the building shake with each blast. This is my reality now.
I arrived in Tel Aviv just before the escalation with a delegation of North American LGBTQ leaders. We came to stand in solidarity with Israel’s LGBTQ community, which has increasingly been isolated by the global queer movement. After the delegation’s five-day mission, I had planned to stay an extra week. But on my first night here, the war broke out.
Despite the fear and chaos, I’m proud to be here. While I’m not a permanent resident of Israel — I live in Los Angeles, home to the largest Iranian Jewish community in the U.S. — I feel like I’m exactly where I’m meant to be. I work in both Iranian and Jewish advocacy spaces, and being here during this pivotal moment is an act of presence, of witness, and of resistance.
The adrenaline of seeing Israel strike back against the IRGC gave way to the sobering realization: I am in a war zone. But I know I’m safer here than I would be in many other places — because Israel protects its people. With shelters. With missile interceptors. With warnings. With a government that values civilian life.
In Iran, people don’t have that. The regime in Iran — and I use that term deliberately, because the regime is not the people — cut off internet access to prevent civilians from receiving IDF warnings before strikes. They wanted maximum casualties. They wanted suffering. They wanted images to manipulate. The same regime that imprisons, tortures, and executes LGBTQ people. The same regime that stripped my family, and millions of others, of their home.
So, when I heard the same anti-Israel activists who have spent the past 20 months calling to “globalize the Intifada” — a clear genocidal chant — adopt the new catchphrase “Hands Off Iran,” my heart sank. This is not solidarity — it’s erasure. These people defend the very regime that forced my parents to flee, tearing our family apart.
Romanticizing the Iranian regime with protest signs and slogans isn’t just tone-deaf. It’s prioritizing aesthetics over truth, trend over substance, and optics over people. It’s especially painful when I see it coming from my LGBTQ peers.
Growing up queer in the Iranian Jewish community during the ’80s and ’90s wasn’t easy. It was LGBTQ spaces that taught me how to stand tall in my truth — how to live authentically and reject shame. But now, those same spaces often turn their backs on me because I’m a Zionist, a widely misunderstood movement which simply calls for Jewish self-determination.
The hypocrisy of the current anti-Israel rhetoric is glaring. The “Hands Off Iran” movement is misguided, providing cover for a regime that tortures its citizens. Yet these activists were nowhere to be found during critical moments like the 2022 “Woman, Life, Freedom” uprisings, when Iranian women risked their lives burning their hijabs in protest. After Mahsa Amini was murdered simply for showing a little hair, those cheering “queers for Palestine” said nothing. This silence in the face of tyranny is not progressive — it’s dangerous.
For me, this conflict is not theoretical — it’s personal. I’ve witnessed firsthand how the Iranian regime targets LGBTQ people, religious minorities, and women. In Israel, I’m free to be who I am — a queer Iranian Jew. If we fail to stand with Israel, we fail to protect the values of freedom, human rights, and dignity. Israel is more than just a country — it’s a refuge for people like me, and it must remain that way.
As I write this, a fragile ceasefire is in place. But even with the quiet, the clarity remains. Israel is more than just a nation. It’s a refuge. And it’s worth standing up for — not because it’s flawless, but because it’s real. And because without it, people like me — queer, Iranian, Jewish — would have nowhere to turn.
Matthew Nouriel is a digital producer at the Tel Aviv Institute, Community Engagement Director at JIMENA, and a queer Iranian Jewish activist. He lives in Los Angeles.
Health
APLA opens eighth location in LA County
The WeHo location is named after Dr. Michael Gottlieb, the groundbreaking physician and researcher who in 1981 co-authored the first medical report identifying AIDS

The Michael Gottlieb Health Center is latest APLA facility to open, making it the eighth location in L.A. County to offer accessible healthcare services.
APLA Health recently opened its brand new the Michael Gottlieb Health Center in West Hollywood with a glitzy ribbon-cutting featuring a bevy of local politicians and community leaders on Friday, June 13. The new location, APLA’ eighth facility, will help the organization provide dedicated LGBTQ-inclusive health services to its more than 22,000 patients.
The new health center boasts 10 exam rooms offering primary, HIV and sexual health care, as well as mental health services. It also includes APLA’s first pharmacy and headquarters for the Alliance for Housing and Healing.
The WeHo location is named after Dr. Michael Gottlieb, the groundbreaking physician and
researcher who in 1981 co-authored the first medical report identifying the illness that
would later become known as AIDS. He later spearheaded important research on the
progression and treatment of HIV/AIDS and co-founded the American Foundation for
AIDS Research. He spent the last four years of his career at APLA, retiring in 2023.
“I’m honored to help dedicate this health center with my name on it,” Gottlieb told a
packed audience in the new center’s waiting room. “The center is named for someone
who is not of the community, but I’m proud to have my name up there, and grateful for a
community that has confided in me and trusted in me for decades now, and I continue
to stand with you in these difficult times in all the issues you’re facing.”
All of the speakers at the opening ceremony noted the difficult political climate for queer
people, immigrants, and health care under the new Trump administration in Washington.
APLA has already been forced to lay off its PrEP Navigation Team from its
Baldwin Hills location, as the federal government has terminated all contracts on HIV
and STD prevention with providers in LA County.
West Hollywood Mayor Chelsea Byers says this moment is an opportunity for the
community to come together to build a strong response.
“We have this opportunity to understand what we are able to do as a local community
against the backdrop of an administration like you had in the 80s,” said Byers. “I wasn’t totally there that whole time. But this link between past experience and present moment is really critical. It’s heartening to see so many community leaders. It’s a really amazing moment we have as a community. At a time when care is needed to be extended to more than ever
before I’m grateful to APLA for making such a beautiful space where care can shine so
bright in our city.”
U.S. Rep. Laura Friedman (CA-30) agreed with that sentiment.
“We have seen this administration deliberately demonize members of our community.
They have demonized immigrants, minorities, our trans community members. They’ve
turned their back on the LGBT community, cruelly cutting funding for AIDS prevention
and STDs. And yet, coming into West Hollywood and this community, and into this
room, we see there’s a tremendous amount of caring and love,” said Friedman. “That is
how we change things in this country, by living those values every day.”
“At a time when the federal government is no longer a partner in anything medical, this
facility is going to provide an incredible and needed safety net for patients,” she said.
Despite these threats, APLA Health CEO Craig Thompson says the organization is
committed to serving everyone who needs care.
“The need for people for health care is going to continue regardless of what the federal
government does around funding, and we’re committed to being there to provide that
health care in all the different ways we possibly can,” he says.
One of the new ways APLA’s new facility will improve service to its patients is through
its new in-house pharmacy.
In addition to fostering closer connection between a patient’s doctor and pharmacist, APLA will offer free delivery at no charge to patients and will help consolidate prescriptions to make it easier for patients to receive and take their medicine.
“We’ve been wanting to close the loop on comprehensive care and offer a pharmacy for
our patients, that way they can get all the support withing one organization,” says Rich
Kowalski, APLA director of pharmacy.
Opinions
Pride and Protests: A weekend full of division
Amid more upcoming raids and protests, we will have to learn when to act, how to react and when to find pockets of joy to celebrate in, because those moments are also acts of resistance

While many Angelenos celebrated the 55th annual L.A. Pride and mainstream news outlets like ABC7 and FOX11 news covered the celebrations, the reality for many other Angelenos involved tear gas, rubber bullets and breaking news coverage from community-led outlets like CALÓ News.
If we were to take a step back into the history of Pride, we would be angered by the amount of violence and pain that led to the protests on the dawn of June 28, 1969. The Stonewall uprising took place as a result of police raids at the now-infamous Stonewall Inn on Christopher Street in New York City. The night that has gone down in history as a canon event for queer and trans life began when police raided the Stonewall Inn and arrested multiple people. The arrests and the police brutality involved, led to an uprising that lasted a total of six days.
Marsha P. Johnson and Sylvia Rivera were credited as being the first people in that historical moment to start the movement we now know and celebrate as Pride. They were Black and brown, people who transformed our notions of fear and action, modeling the mantra that we must act in order to not live in fear. The people at the Stonewall Inn on that night in June all those years ago, and all of the queer and trans people now, have something deeply unsettling in common.
We both live in a constant state of fear and anxiety.
We live in such a major state of fear that anxiety, depression and other mental health issues — including substance abuse disorders — tend to be particularly prevalent in the LGBTQ community. According to Mass Gen, the U.S. is facing a mental health crisis, with nearly 40% of the LGBTQ population in the U.S. reported experiencing mental illness last year, a figure of around 5.8 million people.
Pride began as the very type of protest that went on this past weekend over the U.S. Immigration Customs Enforcement (ICE) raids, where people have been taken into custody, reporters shot with rubber bullets and tear-gassed, and where union president David Huerta was taken into custody and charged with alleged federal conspiracy charges.
Over the weekend, I celebrated Pride. I admittedly celebrated being queer, while my other communities experienced fear in the face of arrests, tear gas to the eyes and baton blows to the head. It was an internal battle I was not prepared for and a real battle on the streets I was not ready to experience. It made me feel weak and more than anything, I felt tired. I felt scared and I felt like I was not prepared for what was to come from these arrests and this violence.
I am a proud child of immigrants. My mother is Colombian and migrated here in the early 80s, settling down in West L.A and building a life with children, houses and her religious community.
My father migrated here in the mid-to-late 80’s from Mexico, where he and his family were hardworking farmers. He has worked at his job, without rest, for over 35 years. He rose up the ranks from line worker to general manager. He does not miss work. He follows every rule and he is never late. Both are documented, but only because of luck and the ease of getting papers back when there weren’t so many bureaucratic steps to gaining citizenship or a green card legally.
My parents and their extended family are proof of a now-distant American Dream, one in which we gain status, we become homeowners and business owners, have children and send them off to college to learn things that our parents can’t even imagine.
Though they did the best they could, my parents had other challenges and barriers to their success. So I worked hard in order to succeed for them. I did it for all of the people in my communities. I did it to raise the statistics on Latinx people, LGBTQ people and former foster youth who go on to college despite the odds and get higher education degrees.
My road to where I am now was paved with uncertainty, food insecurity, homelessness and many other factors that pushed and pulled me back. The analogy I can think of to accurately compare myself to is a catapult. I was pulled down with weights that were added on more and more, until one day I catapulted forward into the life I now have the privilege to live. Though I still struggle in many ways, it is the first time in my life that I am not in survival mode. It’s the first time in my life that I get to exist as a queer person who can enjoy life, build a friend group and establish deep connections with people. It’s also the first time I get to enjoy Pride as someone who is single and who has spent the past 18 months healing from my from my last relationship.
It was the first time in my life, as a lesbian who’s been out for over a decade, that I truly planned to enjoy Pride with my groups of friends.
While I was there this weekend, my internal battle began and I felt torn between celebrating my life and my queerness and covering the ICE raid protests happening not too far from Sunset Blvd.
What I didn’t expect was to see so many other people at Pride, completely oblivious and completely disconnected from the history of Pride, instead glorifying corporate brands and companies that have remained silent over LGBTQ issues, while others have gone as far as rolling back their Diversity, Equity and Inclusion initiatives.
If Marsha P. Johnson or Sylvia Rivera were there at that moment, they would have convinced us to merge our Pride celebration with the protests. They would have rallied us all to join forces, and in the spirit of Pride, we would have marched for our immigrant community members, fighting for their right to due process.
I’m not sure if I made the right decision or not, but the next 60 days will say a lot about every single one of us. We will have to learn when to act, how to react and when to find pockets of joy to celebrate in, because those moments are also acts of resistance.
The Trump administration vowed to strip away rights and has made it their mission to incite violence, fear and anxiety among all working class, BIPOC and LGBTQ people, so it is important, now more than ever, to unite and show up for each other, whether you’re at a Pride celebration or a protest.
The next 60 days will raise our anxiety and fear, but we must remember to also take breaks, celebrate wins, relish in community, hug your loved ones and use whatever amount of privilege that you have, to show up for the communities that are hurting the most in these moments.
Juneteenth is also coming up soon and I hope to see more of us rally around our Black brothers, sisters and siblings, to not only fight for our rights, but to continue celebrating ourselves and each other.
In the words of Marsha P. Johnson: “There is no pride for some of us, without liberation for all of us.”
California
New California trans athlete policy creating ‘co-winners’ is a crock
You didn’t misread that. Hernandez shared the podium with ‘co-winners’
A lot happened at last weekend’s high school state track and field championship meet in
Clovis, Calif. Parents of cisgender student-athletes booed the one and only transgender
girl competing. Police and security officers showed up in large numbers to keep
protestors apart and safeguard the competitors. Police made an arrest outside the
stadium after a demonstrator brandishing a transgender pride flag allegedly assaulted a
man described as a conservative activist and caused damage to his vehicle.
The trans student — 16-year-old AB Hernandez — finished a winner. But she wasn’t “the” winner.
As CBS News reported, “Hernandez took home first place medals in both high jump and
triple jump and she placed second in the long jump event. Following a rule change by
the California Interscholastic Federation, a co-winner was named in each of the three
events in which Hernandez placed.”
You didn’t misread that. Hernandez shared the podium with “co-winners.”
As the Blade reported last week, the CIF introduced a new “pilot entry process” that for
the first time, allowed judges to score trans athletes separately from cisgender
competitors, so there were three winners in every event: a cisgender male winner, a
cisgender female winner and a trans student-athlete winner.
The new policy was announced hours after President Donald Trump threatened to pull
“large scale federal funding” from the state if officials allowed trans athletes to compete
according to their gender identity.
Despite the policy change, the U.S. Department of Justice announced on social
media it was investigating State Attorney General Rob Bonta, State Superintendent of
Public Instruction Tony Thurmond, the Jurupa Unified School District, and the CIF for
potential violations of Title IX, as the Blade reported.
So what happens now? As KXTV reported, President Trump issued another threat to
pull funding on Monday in a post to his Truth Social account, not naming Hernandez but
labeling her “a biological male” and using his favorite derogatory nickname for
California’s Democratic Gov. Gavin Newsom.
“A Biological Male competed in California Girls State Finals, WINNING BIG, despite the
fact that they were warned by me not to do so. As Governor Gavin Newscum fully
understands, large scale fines will be imposed!!!”
Now, the pundits are weighing-in. Sara Pequeño wrote in USA Today how she was
encouraged to see Hernandez share the 2nd place podium with Brooke White and “put
their arms around each other.”
“They’re setting an example for how all of us should treat our trans neighbors, i.e.,
treating them like human beings, not enemies,” she wrote.
As Pequeño noted, Save Women’s Sports, an anti-trans advocacy group, could only
identify five trans students in the entire United States who were competing on girls’
teams from kindergarten through grade 12 in 2023. “That group’s entire existence is to
hate trans athletes, and they found very little to hate,” she wrote.
According to the president of the NCAA, there are fewer than 10 student-athletes
who publicly identify as transgender out of the more than 500,000 competing at the
collegiate level.
Pequeño was not alone in finding joy in the rules change that brought cisgender and
transgender girls together on a podium, each of them a “co-winner.” So did self-
proclaimed “trans advocate” Cyd Zeigler.
He’s one of the co-founders of the LGBTQ+ sports site Outsports, who in 2023
infamously came close to endorsing Florida Republican Gov. Ron DeSantis for
president, only to offer his regrets, following a backlash from readers. Zeigler penned an
op-ed Wednesday originally titled “California trans athlete policy is something everyone
can embrace.”
“Everyone?” Not this sports editor.
He called the new CIF policy “the best possible path in 2025 to trans participation in
sports.”
In celebrating this change, Zeigler also trashed “goal-post-moving trans advocates” and
policies in California and Connecticut that allow “a trans girl to run in boys track meets
and, without a medical transition, later compete in girls meets,” meaning high school
competitions. “That’s bad policy,” declared Zeigler without evidence.
That policy in Connecticut has stood since 2011 and is enshrined in state law, and so far
has withstood legal challenges once again being heard in federal court.
Outsports at some point changed the headline of his screed to “New California trans
athlete policy is something we can embrace” and apparently made another significant
choice: Despite quoting the outlet’s one and only remaining transgender contributor,
Karleigh Webb, who opposes the rules change, Zeigler did not mention her by name.
Why?
In an article published before the championship, Webb wrote: “If AB Hernandez wins,
why should she have to share the spoils with someone else if’s not a tie? That’s what
professional transphobes like Jennifer Sey and Riley Gaines try to sell. Awarding a
duplicate medal gives their nonsense credence to the detriment of the sport and the
athletes.”
Webb is right. Zeigler and the CIF and Gov. Newsom are wrong. You either win, or you
lose, or if you prefer, you come in second, third, whatever. But “co-winners?”
That’s a crock.
Imagine if the Dodgers and Yankees shared the World Series trophy. Why shouldn’t the
49ers also win the Super Bowl alongside the Chiefs? Maybe Kamala Harris should be
declared a “co-winner” of last November’s election?
Personally, I’m glad to see Hernandez embraced by her cisgender peers. I’m relieved to
know that crowds cheering these amazing girls last weekend drowned out the hecklers
who showed up to boo a child. I’m encouraged that even if she had to share the win,
Hernandez was given her rightful place among the teens competing and proved she
was not only worthy of competing but did not win in every event.
So, she’s hardly “unbeatable.” Most trans athletes actually lose, as Zeigler wrote almost
six years ago, back before he started echoing anti-trans inclusion activists Martina Navratilova, Renee Richards and Nancy Hogshead-Makar.
If he really thinks the CIF “co-winners” rule is going to silence anti-trans forces, I think
he’s going to be very surprised by Riley Gaines and her crowd.
While it’s easy for Zeigler to concede public opinion has shifted, he should know
better than to blame those who pushed for inclusion, when it’s clear that conservative
voices in media and politicians, like his, are the ones responsible for influencing that
move to reject trans women’s right to compete in women’s sports. It’s a pendulum swing
that in time will undoubtedly swing back, once the science proves that trans women and
girls don’t always win. In fact, researchers have already proven some trans athletes are
at a disadvantage compared to their cisgender competitors.
Just as Parker Molloy reported that a Republican-commissioned study on gender
affirming care in Utah actually found “that youth who received care before age 18 had
better outcomes, especially around depression, anxiety and suicidality. Hormonal
treatments were associated with positive mental health and psychosocial functioning
outcomes.”
I believe the science is on the side of transgender Americans. Americans love a
winner. Not a “co-winner.”
Opinions
Trump’s inhumanity won’t erase Andry Hernandez Romero, if we resist
Andry Hernández Romero’s case continues to be a violent reminder that we must rise up and resist
Editor’s Note: Since this article was first published, more information on Andry’s case has become available.
UPDATE: On June 4, a federal judge ruled in favor of the ACLU and Democracy Forward in J.G.G. v. Trump, in which deported gay stylist Andry José Hernández Romero is one of the lead plaintiffs. Describing the Venezuelan deportees’ situation as Kafkaesque, Judge James E. Boasberg said the plaintiffs would likely prevail in their complaint about being denied due process, the New York Times reported. Trump officials, Boasberg wrote in his 69-page ruling, “spirited away planeloads of people before any such challenge could be made. And now, significant evidence has come to light indicating that many of those currently entombed in CECOT have no connection to the gang and thus languish in a foreign prison on flimsy, even frivolous, accusations.”
“Absent this relief,” the judge wrote, “the government could snatch anyone off the street, turn him over to a foreign country and then effectively foreclose any corrective course of action.” He ordered the Trump administration to give the deportees the due process they have been denied.
On Friday, June 6, Rep. Pramila Jayapal (WA-07), Ranking Member of the Immigration Integrity, Security, and Enforcement Subcommittee, will host a shadow hearing Kidnapped and Disappeared: Trump’s Lawless Third Country Disappearances at which Andry’s attorney Lindsay Toczylowski will testify.
The juxtaposition is morally excruciating. The very air in West Hollywood is electric with
queer joy and the excitement of WeHo Pride, but it’s more than a celebration of our ongoing
movement for liberation and equality. We’ve been waiting for a moment to exhale and
stop the clamor of the Trump horror show.
What can we do to stop this overwhelming dictatorship campaign that is gleefully
enforcing Project 2025 through a deluge of cruel Executive Orders, demonizing and
erasing anything under Diversity, Equity and Inclusion initiatives and LGBTQ while dispatching masked ICE agents to snatch anyone Trump’s White Supremacist terrorist administration tags for deportation.
Among those swept up in Trump’s frenetic crusade is Andry Hernandez Romero, a 32-
year-old gay hair stylist and makeup artist who fled harassment and threats of violence in Venezuela in May 2024, after speaking out against authoritarian dictator Nicolás Maduro. After navigating the complex app designed to streamline the byzantine U.S. lawful entry process, last August Romero faced a U.S. border official in San Diego. With no criminal history, he demonstrated a “credible fear of persecution” to proceed with an asylum case.
Imagine what Romero felt — so close to freedom, to opportunity, to unabashed queer joy.
Then came that Trumpian twist.
During a physical exam, officials fixated on Romero tattoos of crowns with the words “Mom” and “Dad.” The agent apparently assumed that Venezuelan gangs accept gays because he suspected Andry had gang affiliations and does not fact check because Tren de Aragua does not use crown tattoos for gang identification.
Romero landed in detention awaiting his asylum court date. But one week before the
March 13 hearing in San Diego, Romero was abruptly transferred to a facility in South
Texas, resulting in his absence in court. The hearing was postponed to March 17 when
the immigration judge again asked where Romero was.
“He was removed to El Salvador….we just found out today,” the ICE lawyer replied. The judge questioned the legality of Romero’s deportation without a removal order.
On March 14, Trump invoked the Alien Enemies Act — a 1798 law used during a
declared war — to target immigrants as government “enemies” who had “infiltrated”
America. Secretly, ICE deported Romero and 137 other Venezuelans to El Salvador’s
notorious Terrorism Confinement Center, with Trump paying dictator President Nayib
Bukele to incarcerate the kidnapped immigrants.
The world watched as Andry and his shackled fellow prisoners were displayed on TV
brutally forced off the plane and forced to kneel as agents roughly shaved their heads.
TIME Magazine photographer Philip Holsinger reported that Romero was being slapped while crying out for his mother, “I’m not a gang member. I’m gay. I’m a stylist.”
Trump called the Venezuelans “rapists,” “savages,” “monsters” and “the worst of the
worst,” claiming they were thoroughly vetted. But ProPublica reviewed each case of the
Venezuelan deportees and reported that the Trump administration knew that “the vast
majority” of the 238 Venezuelan immigrants ”had not been convicted of crimes in the
United States before it labeled them as terrorists and deported them, according to U.S.
Department of Homeland Security data that has not been previously reported.”
Lee Gelernt, the American Civil Liberties Union’s lead attorney fighting the deportations,
told ProPublica that the removals amounted to a “’blatant violation of the most
fundamental due process principles” and subjected the deportees to life imprisonment.
There have been numerous attempts to look for a humanitarian bone in the Trump
administration’s body politic, most notably gay immigrant Rep. Robert Garcia’s heated
exchange with Homeland Security Secretary Kristi Noem during a May 14 congressional hearing. Garcia (D-Long Beach) went to El Salvador for a welfare check
but was denied access to Romero.
“He has had no access to lawyers or family since he has been taken over a month now,”
Garcia told Noem. “His mother just wants to know if he is alive.”
“I don’t know the specifics of this individual case. This individual is in El Salvador and
the appeal would be best made to the president and to the government of El Salvador
on this,” replied Noem.
Garcia pushed back.
“You and the president have the ability to check if Andry is alive and is
not being harmed. Would you commit to at least asking El Salvador if he is alive?”
Nope.
“This is a question that’s best asked to the president and government of El
Salvador,” she said.
Noem’s callous disregard for life and suffering is unsurprising. The former governor of
South Dakota blithely noted in her political memoir that she shot and killed her 14-
month-old dog Cricket when the puppy misbehaved. “I hated that dog,” Noem wrote.
She also shot a goat she didn’t like.
“In neither case did Noem show any doubt or remorse; quite the contrary, she sought to
cast her action as a signifier of tough-minded realism that would burnish her appeal as a
politician from a rural community,” wrote Sara Amundson, president of the Humane
Society Legislative Fund.
So if Noem thinks callousness is cool, imagine how she feels about someone she might
deem as sensetive?
“Under the Constitution, every single person has a right to due process, and that means
they have a right to notification of any allegations the government is making against
them and a right to go into court and prove that those allegations are wrong if that’s the
case,” Lindsay Toczylowski, President of the Los Angeles-based Immigrant Defenders
Law Center who is representing Romero pro bono, told NBC News San Diego April 11.
“In Andry’s case, the government never gave us that opportunity. In fact, they didn’t even
bring him to court, and they have forcefully sent him to El Salvador without ever giving
us any notice or without telling us the way that we could appeal their decision.”
On May 27, Immigration Judge Paula Dixon granted a U.S. Dept of Homeland Security motion to dismiss asylum proceedings for Romero scheduled for the following day.
“We should all be incredibly alarmed at what has happened in Andry’s case. The idea
that the government can disappear you because of your tattoos, and never even
give you a day in court, should send a chill down the spine of every American. If this can
happen to Andry, it can happen to any one of us,” said Toczylowski.
Andry’s life depends on us holding the Trump administration accountable for what they
have done to him,” Toczylowski said. “We will continue to fight until Andry is safe and
free.”
Romero is a lead plaintiff in the American Civil Liberties Union’s and Democracy Forward’s J.G.G. v. Trump case in which Romero’s friend and mother gave statements that are now evidence saying Romero “was persecuted both for his sexual orientation and for his refusal to promote government propaganda” while working as a makeup artist at the TV network in Caracas, according to CNN.
But Project 2025 booster Kevin D. Roberts doesn’t care, having ordered the Trump
administration to delete “the terms sexual orientation and gender identity….out of every
federal rule, agency regulation, contract, grant, regulation, and piece of legislation that
exists.”
So do Trumpland judges care about the raison d’etre for asylum or is that too DEI?
NBC News reported that Romero’s dismissal order “allowed for the possibility that the
case be reopened if Hernandez returns to the U.S.”
That’s why we the people, must rise up and resist.
“As the son and grandson of Japanese Americans who were rounded up and forced into
camps without due process, I know all too well that Andry is not the first person to be
unjustly taken by the government,” says out Rep. Mark Takano (CA-39), Chair of the Congressional Equality Caucus. “Every American should be alarmed by how openly the
Trump Administration is taking people off the street and locking them away in a foreign
prison without so much as a day in court — all because of their tattoos. This fight is not
over yet, but every day it drags on puts Andry and others’ lives in danger. I stand with
Andry, his family, his lawyers, and our Constitution in rebuking President Trump’s cruel
and illegal attacks, and hope that justice is swiftly served.”
Longtime activist Cleve Jones urges all LGBTQ people and allies to take action.
“We don’t know if he’s dead or alive,” Cleve says. “I look at [Romero] and he’s like my little
gay brother who is now in this terrible situation where he — if he is still alive — is probably
being subjected to horrendous brutality on a daily basis.”
But Cleve is also angry at the lack of response to this urgently important case.
“If you want to be intersectional and not just quack about it, look at this case,” Cleve
says. “This young man stands at the intersection of our fight for LGBT equality, for
immigrant rights, and for due process under law.”
San Francisco Pride and New York City Pride rejected his request to name Andry an
honorary Grand Marshal. But, Cleve says, “I’m happy that a number of pride
celebrations have done that. Others have stepped up and are organizing fundraisers. I
see there’s one coming up in New York. But everybody should be talking about Andre.
Free Andre. Free Andre. It’s so important!”
Please note: To support Romero’s case and others like it, the Immigrant Defenders Law Center is selling a T-shirt that says “Asylum is a Human Right, found here.“
Health
Brave, Not Broken: Mental health, queer identity and the urgent fight for care
As we near the end of Mental Health Awareness Month, Dr. Greg Cason shares what has changed, what is at risk and why therapy and community matter more than ever

Let’s get one thing straight (well, not too straight), mental health awareness is having its moment — and it’s about damn time.
For LGBTQ+ folks, mental health is not a trend. It is survival. In a time when therapy is finally making its way into casual brunch talk (please stop referring to drinking mimosas as “self-care”), and TikTok is where so many go to share their experiences, we sat down with a psychologist who’s been doing the work long before it was mainstream. Equal parts clinician, advocate and reality TV veteran, Greg Cason offers an authentic and insightful look at queer resilience, the dangerous return of bad policy and why healing often begins with three brave words: I need help.
What does this time signify for you both personally and professionally?
Personally, I am thrilled about how far we’ve come in de-stigmatizing mental health, especially in the LGBTQ community in my lifetime. Professionally, it’s a reminder that my job isn’t just in the therapy room, it’s also about education and advocacy. Social media has helped normalize mental health talk and organizations like National Alliance of Mental Health (NAMI), have been the backbone of that effort. It’s not perfect, but we’ve gone from whispers, to full-blown open dialogues and that’s powerful. But our work is not over.
The current administration in D.C. is taking apart decades of needed research, bringing back discrimination against our LGBTQ brothers and sisters and instituting a “health” agenda based on fringe theories as well as giving voice to influencers over experts. We’ve come a long way, but it’s fragile and if we don’t stand up to the current assaults, we will find ourselves back to the limitations and attitudes that prevailed before most of us were born.
This year’s theme, “Turn Awareness into Action,” emphasizes moving beyond recognition, to tangible change. How can people take meaningful steps to support and promote mental health?
For you personally: start small.
Check in on your friends — really check in. Advocate for better mental health policies at work or school. Normalize therapy. Share your own experiences and together we also need to act. We can’t fall for the constant demonization of members of our own and other communities. We must band together to stand up for the less fortunate and to push back against new assaults. If you truly want to improve your mental health, connect with your community.
What are some common mental health issues faced by queer folks and how does therapy address them?
Higher rates of anxiety, depression, substance use and trauma — much of it rooted in or exacerbated by rejection, discrimination, or internalized shame. Therapy helps untangle those experiences, identify core beliefs, and replace harmful narratives with empowering ones. It’s about rebuilding a sense of self that the world may have tried to tear down.
Even so, therapy is not the only solution. Don’t underestimate the power of community support groups such as Alcoholics Anonymous (AA) and similar organizations. These are powerful resources that not only help you with issues like substance abuse, but also help you to rebuild community and connection.
What’s one myth about queer mental health that you’d like to call out and nip in the bud?
That being LGBTQ causes mental health problems. That’s flat-out wrong. The issue isn’t our identities — it’s the way society treats us. Remove the stigma, support queer folks and the mental health gap shrinks dramatically. But an honorable mention for a rising tide of a disproven and harmful therapeutic approach called “Conversion Therapy.”
Though it promises to change sexual and gender orientation, the only thing it does is shame [LGBTQ people] into silence and produce further trauma. It’s sad when politics and religion drive health priorities without any consideration of science and human functioning.
As a practicing psychologist, how have you seen the conversation around mental health change and evolve, especially within our LGBTQ community?
It used to be shrouded in silence — now it’s becoming part of our culture. I see LGBTQ people openly discussing therapy, boundaries and healing in casual conversations. That’s revolutionary. But I cannot help but think it was born out of necessity.
When AIDS was first identified in 1981, the world also saw therapy as only for those who were mentally ill. But it became a necessity for our community. The ever-present fear of disease and dying was commonplace in our community, combined with the constant assaults from politicians, religious professionals, family, and even friends, we had to identify people that we could open-up to and seek support from.
Those were dark and difficult times and we have progressed in ways that seemed impossible back then. That shift is showing up in the language, the pride, and the resilience of our community.
Your particular practice focuses on Cognitive Behavioral Therapy (CBT). How does CBT serve as an effective tool in addressing mental health challenges in our LGBTQ communities?
I always have to laugh — (CBT) has a very different connotation in our community. But in my world, it stands for the more mundane psychotherapeutic modality. (CBT) is powerful because it helps people understand how their thoughts shape their feelings and behaviors.
That said, it also has a dark past. (CBT) techniques were once used in “Conversion Therapy” to try to change sexual orientation — which is now widely recognized as both unethical and harmful. Today’s (CBT) is different. It’s science-based, jargon-free and focused on helping people recognize and replace harmful beliefs shaped by family, religion, or society.
But it’s not just about thoughts. We also work on behavior change, emotional regulation and achieving goals. It may not sound sexy, but I’ve seen it transform individuals, couples and groups.
I was lucky to do a fellowship with Albert Ellis, one of (CBT’s) pioneers. He taught me two things I always keep close: First, we’re all fallible, fucked-up human beings — and that’s okay. Second, change takes work and practice.
And, as another mentor once said, “change may take a while… so pack a lunch.”
You once starred on Bravo’s LA Shrinks. Did your time in reality television provide you with any new perspectives on psychology or on yourself?
Oh absolutely. Being on “LA Shrinks” was both a wild ride and a mirror (albeit cracked, at times). It reminded me that therapists are human too — flawed, funny, and fully visible. It also deepened my empathy for clients in the public eye. Having your life edited for entertainment is… let’s just say, psychologically complex.
Reality television has become a significant portion of most entertainment and media these days. In what ways and to what scale do you believe it has impacted the mental health of our queer communities?
Reality TV is a double-edged sword. On one hand, it gives visibility to LGBTQ stories — sometimes for the first time. My husband and I were married on the show and that meant so much to me to share that reality with those kids out there like me who grew up without any gay role-models or any hope for a relationship or normal life. On the other, it can flatten people into caricatures. The audience forgets they’re watching a curated narrative — not a whole human being.
I have known some people who were portrayed in a certain way that did not capture their full character, and they suffered as a result. The danger lies in mistaking visibility for authenticity. Reality TV can inform, inspire, or exploit — and often does all three at once. Nonetheless, I cannot tell you how many people said they watch reality TV while they did other things like ironing or laundry. They said it was having their friends with them. That always made me smile.
As someone who’s both a therapist and a public figure, how do you personally stay grounded while continuing to hold space for others?
I have always believed that it is important to leave the therapist at the office. There are people in my profession that don’t allow themselves to be vulnerable in their relationships, silly with their friends, and thrilled to be home alone with a pint of ice-cream and a remote control. We are humans first. So am I. As for anyone approaching me because they saw me on TV or now listen to my podcast, I am always flattered. I realize they are offering me a gift. I don’t have to question the gift or tell them that it is not my size. Rather, my only job is to graciously accept. Doing that has only made my heart grow larger, not my ego.
What advice would you offer to encourage people who hesitate to seek help and begin their journey toward healing?
Therapy doesn’t mean you’re broken — it means you’re brave. Start with one conversation. One resource. One step. You don’t have to commit to a lifetime of therapy — just be open to the possibility that healing is available and that you deserve it.
Looking ahead, what changes or improvements would you like to see in mental health care for the LGBTQ community?
Access, affordability and cultural competency. We need more LGBTQ therapists — and more allies who understand our lived experiences. A personal desire of mine is that therapists focus on science rather than cultural trends or social media diagnoses and treatments. I know the era of social media is making everything a popularity contest. But I hope we can also not forgo expertise just to follow the latest fad.
Whether you’re starting therapy, advocating for others, or simply sharing your story — remember: awareness is only the beginning. Action creates change.
Community Perspectives
‘Protect the dolls’: The viral t-shirt that sparked a movement
The shirt’s message and its impact have turned this moment into a cultural flashpoint

In February 2025, American designer Conner Ives closed his fall and winter show at London Fashion Week with a striking message — not spoken, but worn.
He walked the runway in a T-shirt reading “Protect the Dolls” a phrase that has since gone viral and ignited a wave of support for trans rights around the world. The shirt, now worn by celebrities and activists alike, has become more than a fashion statement — it’s a declaration of solidarity, a tribute to trans dignity and trans rights and a call to action.
“The night before the show, my team and I were sitting around throwing around slogans that we would put on a shirt, which led to Protect the Dolls,” explained Conner Ives in an interview with Trans Lifeline.
The phrase, simple yet powerful, was designed to cut through the noise.
“Maybe the reason that the catchphrase caught on,” said Ives. “Is that rather than coming in with testimonials or facts or percentages… this was maybe a way to simplify down the message to something that could just be said in three words.”
The word “doll” has deep roots in LGBTQ culture, tracing back to the 60s and 70s ballroom scene created by Black and Latino, trans and queer communities. In a world that routinely rejected them, calling each other “doll” was an act of affirmation — a way to celebrate beauty, softness and survival. The term of endearment became a symbol of sisterhood and resistance — a coded language of care in hostile environments. By calling each other dolls, we affirm our beauty, our care and our worth. Like the way societies throughout human civilization have treated cherished dolls — with love, nurture, and tenderness — the term has become a powerful emblem of resistance, sisterhood and self-love.
Today, as trans rights face increasing attacks both in the U.S. and around the world, remembering this legacy feels more urgent than ever. Earlier this year, President Donald Trump, now in his second term, signed multiple executive orders severely restricting transgender rights. Meanwhile, in the U.K., the Supreme Court’s redefinition of “woman” has excluded trans women from key legal protections, marking a major setback for equality. As Ives reflected, “It feels like we are sometimes living in two alternate realities simultaneously… the alternate reality where we have the people that we choose around us, and then the one filled with political theater and hysteria.” In this climate, “Protect the Dolls” is more than a slogan — it’s a rallying cry to defend our rights, affirm our dignity and celebrate the communities we build together.
The shirt’s message and its impact have turned this moment into a cultural flashpoint. Celebrities across fashion, film, music, and social media have rallied around the design, turning their platforms into megaphones for its mission. Pedro Pascal wore it to his 50th birthday party alongside DJ Honey Dijon and again at the European premiere of “Thunderbolts (2025).”
Troye Sivan wore it on stage during Charli XCX’s Coachella 2025 set, where they performed “Talk Talk” together — a redux of their joint tour last year. He later posted a photo wearing the shirt alongside Lorde, Charli XCX and Billie Eilish, further cementing its status as an iconic fashion moment. Other high-profile supporters include Addison Rae, Tilda Swinton, Haider Ackermann, Emma Brooks, bbno$, Lisa Rinna and Camille Charriere — all of whom have proudly shared it on social media. Their posts have helped catapult the shirt into the global spotlight, transforming it into both a fundraiser and a visual rallying cry.
The shirt which sells for £75 (about $99 USD), is available through Ives’s website, with 100% of the proceeds benefiting Trans Lifeline — a nonprofit organization run by and for trans people. Since its launch, over 5,000 shirts have been sold, helping to fund Trans Lifeline’s critical services, including its peer-led crisis hotline and its micro-grants program, which has already distributed over a million dollars directly to trans people.
“I think maybe what really sealed the deal for me was reading the quip somewhere where this is a trans-led U.S.-based charity benefiting trans people,” said Ives.
“I’m not the one picking up the phone helping these people or answering the phones. I think that was really why I wanted that to go where it was going,” he emphasized.
He also emphasized the importance of transparency: “When people say $100 for a T-shirt is a lot, we break down the costs for them. We show them how we’re using organic cotton, fair trade environments, reputable factories—and that over two-thirds of proceeds are going to charity.” Ives even encourages critics to take action however they can: “If the shirt isn’t accessible for you, we tell people: make your own, and donate whatever you can directly to Trans Lifeline.”
What started as a closing runway moment has become a movement. “It feels now like it’s turned into something bigger than just a T-shirt,” Ives reflected. “It’s become a universal concept that is for the people as well. We don’t own that phrase.” In fact, when asked about trademarking Protect the Dolls, Ives responded, “Honestly no, because it’s not mine to own.”
“Protect the Dolls” is more than a fashion statement — it’s a declaration of solidarity and a call to action. Every shirt worn is a stand against the forces that seek to erase us, a tangible investment in a future where trans people not only survive, but thrive. It’s a reminder that our lives, our joy, and our futures are worth fighting for.
Because in the face of systemic violence, we protect each other.
We protect the dolls.
Community Perspectives
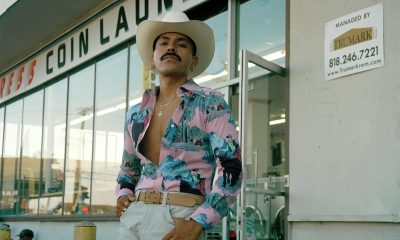
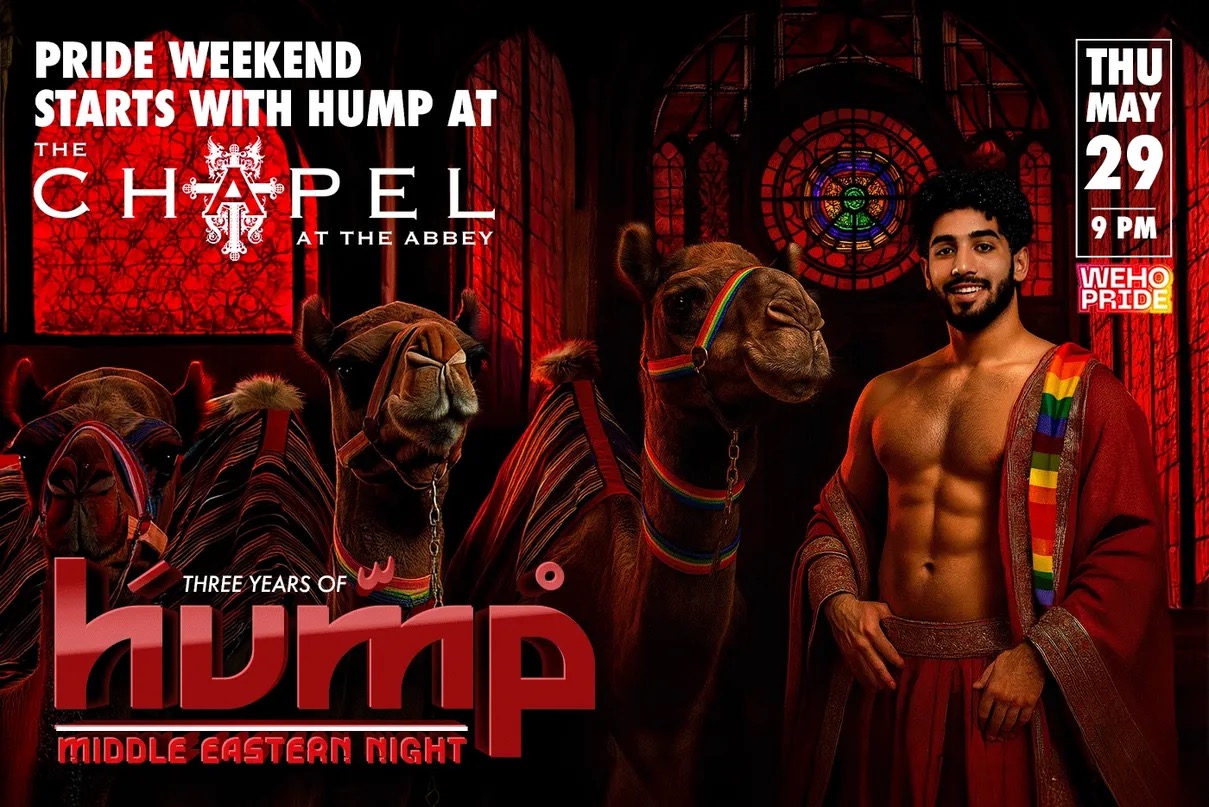
How a promoter brought Middle East Nights to WeHo Gay Bars
Mas is interested in challenging assumptions in the West about sexuality in the Middle East
Mas never meant to become a club promoter. He’s a broad man with a neat beard and twinkling eyes above a grin. After studying marketing and management in the U.S., he returned to the Middle East to help a Dubai company open luxury movie theaters across the region — including the first ever movie theater in Saudi Arabia.
When Covid-19 hit, theaters shuttered and the Lebanese economy crashed. Banks locked people’s money and so, starting over with nothing, he returned to Los Angeles, where he crashed on a friend’s couch for three months.
Ingenuity makes strange bedfellows. When Micky’s in WeHo offered Mas a bartending gig, he pitched the idea of taking over their marketing campaigns instead. Months later, after helping to get the word out about all sorts of different events and evenings, the club asked him if he’d consider hosting a night.
Mas is interested in challenging assumptions in the West about sexuality in the Middle East by hosting this night in the gay-famous WeHo community.
At the time, Mas says, there were no events for the gay Middle Eastern community in L.A., which includes Arabs, Persians and Armenians. The only other gay, Middle Eastern-oriented club was Club Nur, which is now permanently closed. So he thought of hosting his own.
“I wanted to create a space for us to listen to our music,” said Mas. “A place for us to be homesick.”
As a new promoter, the club didn’t offer Mas a weekend, but rather a Wednesday night, which are notoriously difficult to sell. But the day gave Mas the name for his first foray into nightlife.
“They already call it hump day,” he said.
The associations: camels and being horny.
“Save a Camel, Hump a Habibi,” says the screen at the bar, over an image of a shirtless man surrounded by decorative lamps. “Habibi,” is a word in Arabic without an easy translation. The most direct is, “beloved,” or “my dear,” but the part that defies translation is how it means both “friend” and “lover.”
For the first Hump event, the team brought a real live camel to West Hollywood to stand out in front of Micky’s as a photo op.
“To this day that’s what’s remembered,” he said.
People for the Ethical Treatment of Animals (PETA) got wind of what was happening and was not pleased — but Mas explains with an eye roll, that the camel was there for one hour, on an off night, with two trainers and was well looked after.
Mas then spoke about the club promotion politics of that night.
“I was a closeted college student in Louisiana when 9/11 happened,” he said, sharing how his white American friends ran errands for him in the days following the attacks so he wouldn’t run the risk of harassment just for leaving the apartment.
“I still get searched in every airport,” he laughed.
In 2008, he went on America’s Got Talent to perform belly dancing. During his audition, he told the panel that he was there to show the peaceful side of the Middle East and a producer came to him afterward, thanked him for his bravery, and told him that unfortunately they would have to cut his segment from the show for venturing into politics.
“People assume the West is better for gays, but that’s not always true,” he said. “The first experience of homophobia I remember, coming from Lebanon, was while my family was on vacation in Italy.”
“There were five gay clubs in Lebanon growing up,” said Mas. “They were more hidden than here, but they were there.”
He recalls that in Dubai, gay parties happened all the time, but the addresses would be released last-minute to prevent them from being shut down — much like LA’s thriving queer warehouse party scene. People will always find a way.
“In Lebanon, growing up, there was not one type of music.” Lebanon is a crossroads of culture, and influences from Europe and the Middle East mingled freely. “You’d hear English, Spanish, French, and Turkish, even just in how people greeted each other in the street.”
The mix of tunes at Hump parties reflects this vibrant music scene.
I attended Hump at Chapel at The Abbey in March, and the Persian holiday of Nowruz, the new year and start of spring.
“Tonight we’re celebrating the Persian people,” said Mas enthusiastically.
His framework is based on the question: who is being celebrated?
It’s a mixed crowd, and the music oscillates between American pop hits and Persian pop classics. “This one has 3 million Shazams,” exclaimed the similarly clueless white boy next to me when we look up the song that’s playing — which has inspired an eruption of passionate singing-along from the middle of the dance floor. My friend Ruben, who’s from Guatemala, twirls another man through classic Salsa steps, to the Persian beat.
“I don’t know a word, but it still makes me move my hips,” he laughed.
I was pleasantly surprised to find another friend, Ameed, working at the door. His social media feed is a continual anguished cry for his native Palestine, but here he sports a broad grin under his keffiyeh, welcoming people in.
“I never thought something like this could exist,” he said. “I was nervous my first time coming,” Ameed explains how coming out as gay to his family led him to take a step back from his own culture, even to see it as bad or bullying. “Every gay Arab guy has some sort of trauma,” he says. “But here I get to enjoy the parts of my culture I enjoy, while still feeling safe — and I get to meet other people in the same boat.”
When Mas talked about making a space “to be homesick,” I had taken it literally, imagining folks far from where they grew up longing for that homeland. Speaking with Ameed a new meaning dawns on me — the way we are homesick for parts of ourselves that we lose in coming out, or even just in growing up. West Hollywood nightlife is all about selling a fantasy. The fantasy here is of a self-aware person’s internal multitudes can be, even just for an evening, in harmony.
Sometimes that’s just a fantasy. Ameed, who says he works a boring, normal job, offered to staff the door after his last experience where he complimented a doorman on their keffiyeh, and the doorman didn’t know what he was talking about.
“Oh this? They just told me to put it on,” he said.
It’s always a fine line between celebration and appropriation.
Reflecting on how that night was a model queer utopia, I wonder if there’d be enough actual gogos from the Middle East to staff a night like that. Probably not.
The crowd is out in force by 11pm, but, classic Thursday, starts to thin after midnight. I was surprised by the number of women out, seemingly supporting the gay men in their lives.
While Hump started as a part time endeavor, Mas’s production team now puts on a slew of gay nights at various bars, including Barbearians (think lots of fur and leather, a play on the erotics of “savagery”) as well as, Steam, a bathhouse-themed night in which guests are encouraged to wear only a towel at the bar. While not specifically Middle Eastern, these nights have the fingerprints of their progenitor, from the music played to, at Steam — a Hookah station where guests can smoke water pipes outdoors and send up smoke like the steam at a bathhouse.
These parties have grown, now touring other cities and even bringing a float to WeHo Pride complete with a flying carpet and gay influencers from Iran, Tunisia, and Iraq. Barbearians, now entering its second year, recently hosted its first Mr. Barbearian competition, which will send the winner, Dé Hanno, to represent the event at Mr. International Leather in Chicago. There’s also intercultural collaborations, like Yalla Papi, a Middle Eastern and Latino night that blends the music of both cultures.
“Latinos move their hips side to side, Arabs move them up and down,” said Mas cheekily.
Mas stated that his goal is to foster a sense of cosmopolitanism and inclusivity. Hump and its progeny provide a safe space for queer Middle Eastern men and their allies to express their sexuality, but also create a meeting ground on their “home turf,” that challenges cultural conceptions both internally and externally.
California
Long Beach Pride reaffirms community focus for this year’s festival
This year’s theme is ‘Power of Community’

Long Beach Pride 2025 will take place on May 17 and 18 at Marina Green Park, emphasizing focus on grassroots organizations and local community performers.
“Long Beach Pride has always been more than just a festival—it’s a movement,” said Elsa Martinez, interim president of LB Pride. “This year, more than ever, we’re celebrating the strength, creativity, and unity of our local community.”
Martinez also notes that all the ticket sales directly go toward funding on-the-ground resources.
“As a nonprofit organization, every aspect of the Pride Festival—from ticket sales to vendor partnerships—directly funds our work in the community,” noted Martinez. “This is a festival with purpose.”
As LB Pride amps up for its 42nd annual celebration, the organization has stated that this year marks the return to the roots of Pride. LB Pride stated that they are committed to emphasizing what makes the local community so special and spotlighting local performers, musicians and entertainers.
The organization has also stated that they are committed to ‘justice, inclusion, and the celebration of queer joy.’
“Our strength has always been our solidarity,” said Martinez. “This year’s festival is a reminder of what we can achieve when we lift each other up.”
This year, the main stage will feature a lineup of pop, Hip-hop and Latin talent.
Performers include HYM the Rapper, George Michael Reborn Tribute, Tori Kay, Jewels Drag Show Extravaganza, Secret Service, Tiancho and music mixes by DJ BSelecta, DJ Icy Ice and DJ 360.
For updates, tickets, and volunteer opportunities, please visit https://longbeachpride.com and follow @LongBeachPride on social media.

Breaking the mental health mold with Ketamine: insights from creator of Better U

Can you really find true love in LA? Insights from a queer matchmaker

Intuitive Shana gives us her hot take for July’s tarot reading

Koaty & Sumner: Finding love in the adult industry

Major victory for LGBTQ funding in LA County
Major victory for LGBTQ funding in LA County
Koaty & Sumner: Finding love in the adult industry
Breaking the mental health mold with Ketamine: insights from creator of Better U
Can you really find true love in LA? Insights from a queer matchmaker

La marcha LGBTQ+ desafía el silencio en El Salvador
-
 Breaking News3 days ago
Breaking News3 days agoMajor victory for LGBTQ funding in LA County
-
 Features3 days ago
Features3 days agoKoaty & Sumner: Finding love in the adult industry
-
 Commentary1 day ago
Commentary1 day agoBreaking the mental health mold with Ketamine: insights from creator of Better U
-
 Miscellaneous2 days ago
Miscellaneous2 days agoCan you really find true love in LA? Insights from a queer matchmaker
-
 El Salvador3 days ago
El Salvador3 days agoLa marcha LGBTQ+ desafía el silencio en El Salvador
-
 Arts & Entertainment2 days ago
Arts & Entertainment2 days agoIntuitive Shana gives us her hot take for July’s tarot reading