
Commentary
The importance of prostate cancer screening: my story
My diagnosis reconfirms my commitment — as an activist, a journalist and a radio host — to fight for access to health care for everyone.

By Michelangelo Signorile | NEW YORK – I was recently diagnosed with prostate cancer. And I’m going to be fine.
Fortunately, it’s localized, and it’s been detected early — so early that I don’t require treatment right now beyond what is called active surveillance, which means monitoring how fast, or how slowly, it grows. If and when I do require further treatment there are options and it is curable.
All of that said, I can’t tell you that the past few weeks have not been a bit excruciating.
Waiting two weeks for biopsy results is living in a cesspool of anxiety. Finding out the news that you have cancer is a gut punch, particularly before you know many of the details. But learning all the facts is key to feeling in control of the situation.
I want to explain what happened so that maybe it can help other people, particularly with regard to the vital importance of early detection.
Back in February, I went for my annual physical and it turned out my levels of PSA — prostate-specific antigen — were slightly-elevated. For those who don’t know, this is a number determined via a routine blood test. I had no symptoms of prostate cancer. No physical exam showed anything out of the ordinary. Even a sonogram was normal.
Sometimes PSA levels in the blood can spike a little bit from working out a lot, and particularly from riding a bike. And some people just have higher levels at a given point, or develop PSA levels that bounce up and down. I could have been in those categories.
So, my doctors and I waited six months and did another PSA test. The number was slightly more elevated.
Only 25% of people with slightly elevated PSA levels, but no symptoms or indications via a digital rectal exam, turn out to have prostate cancer. There are other less serious health issues — such as a urinary tract infection — that can cause the number to be elevated.
The next step should have been an MRI. But my insurance company wouldn’t pay for it because nothing else beyond my slightly-elevated PSA levels indicated prostate cancer. In other words, I didn’t appear sick enough to find out how sick I was. This is another reason why health insurance is a disaster. In case you needed another reason.
So I had a biopsy. It wasn’t that bad, actually. Fifteen to 20 minutes in the urologists’s office, and done. Local anesthesia and some valium. Slight discomfort but no real pain.
Then the wait. And then the phone call from my urologist, after which my heart sank.
But I felt almost 100% better after my husband David and I went into the office, where my urologist explained it was found early and showed us precisely where it was limited to in the prostate. Finally, he said he fully anticipated a CT scan and a whole-body bone scan would show it had not spread beyond the prostate. (Both scans, performed a week later during a full day in a hospital, confirmed his belief.) My friend Joe had advised me to record the meeting with the doctor because I would be so overwhelmed I’d forget just about everything. My mother thought that was such smart advice, and she was right.
Active surveillance — basically, monitoring the PSA numbers via a blood test every few months — is actually now considered a treatment. If and when I require or would like further treatment, there are choices, different options with excellent outcomes. I have time to research them and weigh them, and get other opinions.
Having that ability can in large part be attributed to early detection.
“Friends” star James Michael Tyler, who famously played Gunther, tragically died this week due to prostate cancer at the age of 59. Tyler appears to have a had a much more aggressive form of prostate cancer. But early detection still would have made a difference. The cancer had already spread to his bones by 2018 when he had his very first PSA test, which showed staggeringly high levels of PSA in his blood. Tyler said he should have “listened to my wonderful wife” and gotten tested sooner:
I would have gone in earlier, and it would have been, hopefully, caught earlier. The next time you go in for just a basic exam or your yearly check-up, please ask your doctor for a PSA test. Caught early, 99 percent treatable.
So I want to take this opportunity to urge everyone who has a prostate and isn’t getting PSA-tested to speak with your doctor about regularly getting a PSA test. I’ve now learned that some doctors advocate regular screening when patients turn 40 while other doctors don’t test at all, even among older patients, unless a patient requests it.
The Prostate Cancer Foundation recommends screening beginning at 40 if you are Black, or have a family history of prostate cancer. And beginning at 45 for everyone else. The American Cancer Society says screening should begin at 50, and at 45 if you’re Black, or there is a family history. The U.S. Preventive Services Task Force recommends talking to your doctor about screening beginning at 55 (and only screening until age 69).
These differences in recommendations have caused confusion. They stem, for the most part, from concerns among medical professionals about too many unnecessary biopsies and over-treatment. So, if your doctor hasn’t already decided to regularly screen you (and I’m thankful that mine did) you have to make the decision for yourself and ask about it. It’s just a blood test. It can’t hurt you. But it can save your life.
You should also be getting a routine digital rectal exam (DRE), which takes just a minute. Some doctors don’t perform it. Some patients don’t like to have it done. Get over it. Sometimes PSA levels will reveal a problem while a DRE doesn’t show it (as in my case). But in other instances a DRE will indicate an issue that a PSA test doesn’t reveal.
Let me repeat: I had —and still have — no symptoms. I feel great, and am in otherwise excellent physical condition. I’m very active and workout at the gym or run outside just about every day. I’ve been vegetarian for over 30 years. So don’t think you’re too healthy, or that you’d feel ill or would have some other indications.
I’m sure many of you have been down this road, or are on it now, and will have a lot to add. I’m grateful for your thoughts and experiences. Certainly queer people of my generation lived through the early HIV epidemic and empowered ourselves, learning that information is power. My experience as an AIDS activist has taught me a lot and I’m confident it’s prepared me for this.
I’ve already come to realize, for example, how straight men and gay men, as well as transgender women, are faced with uniquely different sets of challenges when it comes to prostate cancer treatments, possible side effects affecting sexual health and other issues. And you can guess which group the medical field is often more geared toward focusing on.
I consider myself very lucky. I benefited from early detection. I live in a city with the best doctors and medical technology in the world. And I have comparatively good health insurance, headaches and ridiculousness notwithstanding.
It means very little to tell people to get PSA-tested if they are uninsured and don’t have adequate medical care. And that is the case for millions of Americans. My diagnosis reconfirms my commitment — as an activist, a journalist and a radio host — to fight for access to health care for everyone.
*******************

Michelangelo Signorile is an American journalist, author and talk radio host. His radio program is aired each weekday across the United States and Canada on Sirius XM Radio and globally online.
Signorile is noted for his various books and articles on gay and lesbian politics and is an outspoken supporter of LGBTQ+ rights. He became a gay activist in 1988, after attending a meeting of the grass roots protest group, ACT UP, in New York. Signorile rose to national prominence as a columnist and writer for OutWeek magazine where he ‘outed’ closeted public figures who were working against the LGBTQ+ community.
Signorile was inducted into the National Lesbian and Gay Journalists Association LGBT Journalist Hall of Fame in 2011.
********************
The preceding article was previously published at The Signorile Report and is republished by permission.


Commentary
Why fans ‘complete’ the Storrie: The psychology behind RPF & fandom narratives
Fans’ projections and invented narratives can blur the line between perception and reality. This constant scripting can compound emotional strain and stress, influencing celebs’ sense of self and mental well-being.

There comes a moment in modern fame when admiration is no longer a simple applause or the overly enthusiastic fan page. No longer satisfied with merely watching and reading about celebs, fans today narrate them, reinterpret them, and renovate them like HGTV contractors with unaddressed attachment issues. Enter “real person fiction” (RPF), where our hottest reigning celebs are transformed into protagonists in elaborate romantic epics written by nameless fans with Tumblr accounts and suspiciously elevated emotional vocabularies.
Queue Heated Rivalry stars Hudson Williams and Connor Storrie, two guys who have discovered that success no longer means simple invites to the (decaying) Met Gala. It means becoming narratively available. These two repeatedly find themselves pulled into the far too familiar fandom dynamic that is born from perceived contrast in personality and charisma. Fans tend not just to observe these relationships but to “complete” them by filling in narrative gaps with their own projections.
Freud, who would have had the time of his life on fan fiction platforms like Archive of Our Own, would likely argue that RPF is fundamentally wish fulfillment disguised as storytelling. In The Interpretation of Dreams, he suggests that fantasies give way to the safe expression of otherwise repressed desires. Fanfiction functions in a similar fashion in that it creates a socially sanctioned dream space where readers and writers can explore longing, intimacy, conflict, identity, vulnerability, and power, all while pretending this is somehow about hockey players or actors and not, say, one’s inability to emotionally communicate after yet another situationship gone south.
The allure of celebrity culture is that it provides emotionally resonant raw material without requiring reciprocal intimacy. Fans “know” just enough to feel attached, but not enough to shake the fantasy. Williams smiles in interviews. Storrie touches his shoulder at a premiere. The human brain, tragically devoted to pattern recognition, immediately starts drafting narrative fantasy.
Parasocial attachment, the one-sided emotional bond audiences form with public figures, has existed for eons. But social media has amped it up into something approaching communal mythmaking. Fans are no longer consuming celebs passively. They collaborate in interpreting them. TikTok vids, Reddit reads, Twitter threads with forensic-level scrutiny of a mere side-glance, modern fandom looks less like a fan club and more like a writers’ room on Adderall.
Traditional romance narratives involve imagined characters. RPF holds the yummy illusion of possibility. Even when readers know intellectually that stories are fictionalized, the existence of real bodies beneath the fantasy creates additional emotional charge. It feels equal parts forbidden and authentic. Freud would likely call this the eroticization of proximity and taboo. The online community calls it ‘shipping.
But dismissing RPF entirely as “crazy fandom behavior” misses the point. Most of those who indulge in it understand boundaries perfectly well. Most know the stories are fantasy constructions. Most are neither delusional nor malicious. They are engaging in a fundamentally human activity of storytelling as emotional management. That said, and this is where things become ethically blurred, healthy projection can drift into possessiveness before we realize it.
The internet promotes excess. Casual recognition turns into “stanning.” Stanning becomes stalking. Every celebrity interaction becomes evidence. Fans begin to experience emotional entitlement toward people they do not actually know. The line between “I dig this dynamic” and “I demand this dynamic validate my emotional investment” grows thin. For celebrities like Williams and Storrie, the psychological burden of this must be deeply strange because, unlike fictional characters, they do not have the option of stepping away from the narrative.
There is likely a destabilizing dissociation that perhaps inevitably develops with such an experience. One may become hyper-aware of their performative self. Every interaction is perceived as being at risk of symbolic overinterpretation. Public identity could potentially fracture (leave Britney alone!) The actual self, the media self, the fandom self, and the fanfiction self. Celebs increasingly live beside fictional doubles birthed from collective desire.
So, how can public figures cope with this healthily? For starters, implement boundaries without contempt. Celebs don’t owe fans unrestricted emotional access, but publicly putting down fandom doesn’t quite work either. Mockery often increases attachment because fans experience criticism as an invalidation of community. Perhaps more effective methods involve calm boundary-setting like refusing to respond to invasive questions, limiting social media exposure, and nourishing strong offline identities rooted in relationships untouched by public consumption. Public figures need protected spaces of non-performance.
Williams and Storrie, hypothetically speaking, would likely benefit from recognizing that most fan projection is not actually about them personally but rather what they represent. Once you understand yourself as an archetype in public consciousness rather than merely an individual, fandom behavior becomes less uniquely cringe and more anthropologically inevitable.
As for our fan girlies, perhaps the healthier future of fandom lies not in less enthusiasm but in more differentiation. One can appreciate lens-fogging chemistry without the demand for portraying the illusion off-camera. It is possible to write fiction inspired by public figures while remembering that those same figures have private lives that you are in no way, shape, or form entitled to.
Freud believed civilization itself relies on sublimation: transforming raw desire into socially productive expression. In this sense, fandom, at its best, is sublimation in action, repurposing loneliness and desire into creativity and community. At its worst, however, sublimation collapses back into good ol’ overconsumption.
The challenge, then, for modern fandom is not throwing out fantasy entirely. Human beings will always fantasize. We are storytelling primates with attachment disorders and Wi-Fi. The challenge is retaining enough humility to remember that behind every projection screen stands an actual person who did not consent to becoming the main character in your collective unconscious, no matter how swoon-worthy they are in a jockstrap.
Ghana
Intersex lives, constitutional freedom, and the dangerous future of Ghana’s Human Sexual Rights and Family Values Bill
Lawmakers continue to consider draconian measure

There is a dangerous silence surrounding intersex lives in Ghana — a silence shaped by fear, misinformation, cultural misunderstanding, and institutional neglect. Today, amid discussions around the possible passage of the Human Sexual Rights and Family Values Bill, 2025, that silence risks becoming law, reinforcing exclusion and deepening the marginalization of already invisible lives.
Much of the national debate surrounding the bill has focused on LGBTQ+ identities. Yet buried within it are implications for intersex persons that many Ghanaians do not fully understand because intersex realities remain largely invisible.
Intersex persons are born with natural variations in chromosomes, hormones, reproductive anatomy, and/or genital characteristics that do not fit typical definitions of male or female bodies. Intersex is not a sexual orientation or gender identity. It is a biological reality. Ghana’s Commission on Human Rights and Administrative Justice (CHRAJ) has clearly acknowledged this distinction.
Despite this distinction, the bill mistakenly collapses intersex realities into a legal framework linked to LGBTQ+ criminalization.
Although the bill contains only limited references to intersex persons, under certain medical exceptions, these references do not amount to recognition or protection. Instead, they frame intersex bodies as abnormalities requiring regulation, correction, and institutional management. This approach is inconsistent not only with Ghana’s constitutional guarantees of dignity, equality, privacy, and liberty, but also with emerging African and international human rights standards. The African Commission on Human and Peoples’ Rights Resolution on the Promotion and Protection of the Rights of Intersex Persons in Africa – ACHPR/Res.552 (LXXIV) 2023 affirms protections relating to bodily integrity, dignity, freedom from discrimination, and against harmful medical practices. Additionally, the United Nations has repeatedly condemned medically unnecessary and non-consensual interventions on intersex children. Rather than affirming the humanity and autonomy of intersex persons, the bill risks legitimizing systems of surveillance, coercion, violence, and institutional erasure.
This is not protection.
It is managed erasure.
A child born intersex in Ghana already enters a society shaped by secrecy and stigma. Families are often pressured to hide intersex children or seek “correction” to make their bodies conform to social expectations.
The bill risks intensifying this pressure.
Clause 17 creates space for “approved service providers” to support interventions relating to intersex persons, yet offers little protection around informed consent, bodily autonomy, confidentiality, or coercive treatment. Under the language of “correction” or “support,” harmful interventions may become normalized.
The intersex community has documented painful lived experiences of intersex Ghanaians that reveal the devastating consequences of stigma and invisibility.
One heartbreaking case involved intersex twins born in Ghana’s Eastern Region in 1993, who were repeatedly forced to move from village to village because of rejection and ridicule. After losing their father, their main source of protection and support, they became even more vulnerable and reportedly experienced severe emotional distress, including suicidal thoughts linked to years of stigma and exclusion. This is what invisibility looks like in practice.
Another painful example is the story of Ativor Holali, whose lived experience exposed the cruel realities intersex persons face in sports and public life. Ativor Holali endured invasive scrutiny, public humiliation, and social suspicion because her body did not conform to rigid expectations of femininity. Rather than being protected as a Ghanaian athlete deserving dignity and privacy, she became the subject of speculation, gossip, and institutional discomfort.
Her experience reflects a broader social crisis: when society insists that every body must fit a narrow binary definition, intersex people are forced to defend their humanity in spaces where dignity should already be guaranteed.
Intersex Persons Society Of Ghana (IPSOG)’s Ŋusẽdodo research further revealed that approximately 70 percent of intersex respondents reported depression, anxiety, trauma, or severe emotional distress linked to medical mistreatment, family rejection, bullying, and social exclusion.
The bill risks transforming these existing prejudices into institutional policy. Several provisions risk deepening surveillance, restricting advocacy, weakening confidentiality, and discouraging public education around intersex realities. Intersex-led organizations providing healthcare guidance, legal referrals, psychosocial support, and community services may face serious challenges.
This places IPSOG and other intersex-led organizations in Ghana at serious risk.
For many intersex Ghanaians, these spaces are not political luxuries.
They are survival mechanisms.
Governments derive legitimacy by protecting the natural rights of all persons, including dignity, liberty, bodily autonomy, and freedom from arbitrary interference. The bill raises concerns because it risks weakening these protections for intersex persons through surveillance, coercive interventions, and restrictions on advocacy.
Ghana’s Constitution declares that “the dignity of all persons shall be inviolable.” Articles 15, 17, 18, and 21 specifically protect dignity, equality, privacy, expression, and freedom of association. These protections should apply equally to intersex persons.
Intersex persons are not threats to Ghanaian culture.
Intersex children are not moral dangers.
Intersex bodies are not political weapons.
They are human beings deserving dignity, healthcare, safety, and constitutional protection.
The true measure of a democracy is how it protects those most vulnerable to exclusion. At this moment, Ghana faces a choice: deepen fear and silence, or uphold dignity, bodily autonomy, and constitutional freedom for intersex persons.
History will remember the choice we make.
Fafali Delight Akortsu is the founder and president of the Intersex Persons Society of Ghana (IPSOG).
Commentary
LGBTQ+ Angelenos need to vote in June – and choose ‘Yes’ on Measure ER
Measure ER would backfill the cuts to HIV and gender affirming care, as well as fund the Planned Parenthood clinics, community health centers, public hospitals, and emergency rooms that many of us depend on.

By Jim Mangia, president and CEO of St. John’s Community Health
As someone who has spent more than twenty-five years working in public health, I’ve seen the devastating impact of people being denied basic medical care because of politics, stigma, or indifference. And as a gay man who came of age in Greenwich Village during the AIDS crisis, I deeply understand what happens when institutions decide certain communities are expendable.
I watched friend after friend die from AIDS while the federal government did nothing, and while much of heterosexual society looked away – or even applauded our suffering. The mass death of LGBTQ+ people was treated as acceptable collateral damage. That era taught me a lesson I have carried throughout my career: when public health systems are weakened, marginalized communities suffer first and worst.
That is why I am deeply alarmed by what is happening in Los Angeles County today.
Because of the Trump administration’s cuts through H.R. 1 — the big, ugly bill — Los Angeles County is projected to lose $2.4 billion in health care revenue over the next three years. Those cuts are already destabilizing the public health infrastructure that millions of Angelenos rely on every day. Additionally, the Trump administration has already slashed federal grant funding for HIV testing and treatment, gender affirming health care, and many other programs critical to the LGBTQ+ community.
But voters have a chance to stop the bleeding.
This June, Los Angeles County voters can pass Measure ER, a temporary funding measure that would generate approximately $1 billion annually to stabilize our health care system. For LGBTQ+ Angelenos in particular, the stakes could not be higher. Measure ER would backfill the cuts to HIV and gender affirming care, as well as fund the Planned Parenthood clinics, community health centers, public hospitals, and emergency rooms that many of us depend on.
The destabilization is already happening. Earlier this year, seven of the Los Angeles County Department of Public Health’s thirteen clinics were forced to close because of severe funding shortfalls. Those clinics provided free or low-cost STI testing and treatment, vaccinations, HIV prevention services, and other essential care. And 200,000 Angelenos have already been disenrolled from Medi-Cal, with at least a million more expected to lose coverage if we don’t act now.

We know what happens when access to preventive care disappears. HIV infections rise. STIs spread more rapidly. Preventable illnesses become emergencies. People delay treatment until they are critically sick, simply because they cannot afford to go to the doctor.
The danger is especially acute for transgender Angelenos. Across the country, the Trump administration and Republican-led states have launched relentless attacks on transgender people. Even here in California, some hospitals and health systems began scaling back gender-affirming services at the first sign of federal scrutiny.
Meanwhile, the Trump administration continues attempting to collect private information related to gender-affirming care nationwide. Luckily, California officials are refusing to give in to this alarming overstep. We must join them in fighting federal attacks on our lives.
If our public health system collapses, transgender folks, low-income people, undocumented communities, seniors, and LGBTQ+ youth will all face even greater barriers to care. And when medical care becomes inaccessible, desperate people often turn to dangerous alternatives. We cannot allow that to happen.
Now, I understand the hesitation some feel when they hear the word “tax.” Frankly, I share some of that frustration myself. Californians already pay a great deal in taxes, and many people are struggling.
But health care is a huge affordability issue. If people lose Medi-Cal and can’t manage their chronic conditions, they can’t work. Then, they can’t pay their rent. Then, more people are forced onto the streets.
Plus, if uninsured people delay treatment and end up in the hospital for a preventable illness, the cost to taxpayers down the line is far greater than the temporary half-penny Measure ER asks for. If we don’t prevent the collapse of our county’s health care infrastructure, people with private insurance will see significantly higher premiums and reduced benefits. That’s because when health providers take on more unpaid care by treating uninsured people, those costs shift to commercial insurers, who then pass the costs onto consumers. All while wait times become longer, appointment times become shorter, and specialized care becomes harder to find.
In my view, half a penny is a reasonable response to the largest health care cuts in the history of the United States – especially given that groceries, prescriptions, and medical equipment are all exempt from the extra half cent.
Measure ER was well planned. It includes a sunset provision, meaning the tax automatically expires after five years. The funding has also already been designated for specific purposes: community clinics, public hospitals, emergency medical services, and providers like Planned Parenthood. Oversight provisions and an advisory committee are also built in to help ensure the money goes exactly where it is supposed to.

For decades, LGBTQ+ communities have fought to be treated with dignity by our health care system. We organized when the government ignored AIDS. We built networks of care when doctors refused to treat transgender patients. We demanded visibility, funding, research, treatment, and compassion because our lives depended on it.
As my friends died all around me during the AIDS pandemic, I advocated in the streets, with tens of thousands of my sisters and brothers, for lifesaving funding. Now, we are once again being asked to defend the public infrastructure that keeps our communities healthy and alive.
We must ask ourselves: Will we allow federal attacks on public health to dismantle decades of hard-fought progress in LA County? Or will we fight back, like we always have?
LGBTQ+ Angelenos have both an opportunity and a responsibility this June. I urge voters across Los Angeles County to organize their families, friends, neighbors, and communities to vote yes on Measure ER.
Our health care system — and countless lives — depend on it.
Commentary
‘Live Your Pride’ is much more than a slogan
Waves Ahead forced to cancel May 17 event in Puerto Rico
On May 5, I spoke by phone with Wilfred Labiosa, executive director of Waves Ahead, a Puerto Rico-based LGBTQ+ community organization that for years has provided mental health services, support programs, and safe spaces for vulnerable communities across the island. During our conversation, Labiosa confirmed every concern described in the organization’s public statement announcing the cancellation of “Live Your Pride,” an event scheduled for Sunday in the northwestern municipality of Isabela. But beyond the financial struggles and organizational challenges, what stayed with me most was the emotional weight behind his words. There was pain in his voice while describing what it means to watch spaces like these slowly disappear.
This was not simply the cancellation of a community event.
“Live Your Pride” had been envisioned as a celebration and affirming gathering for LGBTQ+ older adults and their allies in Puerto Rico. In a society where many LGBTQ+ elders spent decades hiding parts of themselves in order to survive, spaces like this carry enormous emotional and social significance. They become places where people can finally exist openly, without fear, apology, or shame.
That is why this cancellation matters far beyond Isabela.
What is happening in Puerto Rico cannot be separated from the broader political climate unfolding across the U.S. and its territories, where programs connected to diversity, inclusion, education, mental health, and LGBTQ+ visibility increasingly find themselves under political attack. These changes do not always arrive through dramatic announcements. More often, they happen quietly. Funding disappears. Community organizations weaken. Safe spaces become harder to sustain. Eventually, the absence itself begins to feel normal.
That normalization is dangerous.
For years, organizations like Waves Ahead have stepped into gaps left behind by institutions and governments, particularly in communities where LGBTQ+ people continue facing discrimination, social isolation, economic instability, and mental health struggles. Their work has never been limited to organizing events. It has involved accompanying people through loneliness, trauma, rejection, depression, aging, and survival itself.
“Live Your Pride” represented much more than entertainment. It represented visibility for LGBTQ+ older adults, many of whom survived decades of family rejection, religious exclusion, workplace discrimination, violence, and silence. These are individuals who came of age during years when living openly could cost someone employment, housing, relationships, or personal safety. Many learned to survive by making themselves invisible.
When spaces like this disappear, something deeply human is lost.
A gathering is canceled, yes, but so is an opportunity for healing, connection, recognition, and dignity. For many LGBTQ+ older adults, especially in smaller municipalities across Puerto Rico, these events are not secondary luxuries. They are reminders that their lives still matter in a society that too often treats aging and queer existence as disposable.
There are still political and religious sectors that portray the rainbow as some kind of ideological threat. But the rainbow does not erase anyone. It illuminates people and stories that society has often tried to ignore. It reflects the lives of young people forced out of their homes, transgender individuals targeted by violence, older adults aging in silence, and families that spent years defending their right to exist openly.
Perhaps that is precisely why the rainbow unsettles some people so deeply.
Its colors expose abandonment, hypocrisy, inequality, and fear. They force societies to confront realities that are easier to ignore than to address honestly. They reveal how fragile human dignity becomes when political agendas decide that certain communities are no longer worthy of protection, funding, or visibility.
The greatest concern here is not solely the cancellation of one event in one Puerto Rican town. The deeper concern is the message quietly taking shape behind decisions like these — the idea that some communities can wait, that some lives deserve fewer resources, and that safe spaces for vulnerable people are expendable during moments of political tension.
History has shown repeatedly how social regression begins. Rarely with one dramatic act. More often through exhaustion, silence, budget cuts, and the slow dismantling of organizations doing essential community work.
Even so, Waves Ahead made one thing clear in its statement. Although “Live Your Pride” has been canceled, the organization will continue providing mental health and community support services through its centers across Puerto Rico. That commitment matters because people do not survive on slogans alone. They survive because somewhere there are still open doors, trained professionals, supportive communities, and people willing to remain present when the world becomes colder and more hostile.
Puerto Rico should pay close attention to what this moment represents. No healthy society is built by weakening the organizations that care for vulnerable people. No government should feel comfortable watching community groups struggle to survive while attempting to provide services and compassion that public institutions themselves often fail to offer.
The rainbow has never been the problem.
The real problem is the discomfort created when its colors force society to confront the wounds, inequalities, and human realities that too many people would rather keep hidden.
Commentary
He is 16 and sitting in a Cuban prison
Jonathan David Muir Burgos arrested after participating in anti-government protests

Jonathan David Muir Burgos is 16-years-old, and that fact alone should force the world to stop and pay attention. He is not an armed criminal, nor a violent extremist, nor someone accused of harming others. He is a Cuban teenager who ended up behind bars after joining recent protests in the city of Morón, in the province of Ciego de Ávila, demonstrations born out of exhaustion, desperation, and the growing collapse of daily life across the island.
Those protests did not emerge from privilege or political theater. They erupted after prolonged blackouts, food shortages, lack of drinking water, unbearable heat, and a level of public frustration that continues to deepen inside Cuba. People took to the streets because ordinary life itself has become increasingly unbearable. Families are surviving for hours and sometimes days without electricity. Parents struggle to find food. Entire communities live trapped between scarcity and silence.
Jonathan became part of that reality.
And today, he is sitting inside a Cuban prison.
The World Health Organization defines adolescence as the stage between approximately 10 and 19 years of age, a period marked by emotional, psychological, and physical development. That matters deeply here because Jonathan is not simply a “young protester.” He is a minor. A teenager still navigating the fragile years in which identity, emotional stability, and personal growth are being formed.
Yet the Cuban government chose to place him inside a high-security prison alongside adults.
There is something profoundly disturbing about a political system willing to expose a 16-year-old boy to the psychological brutality of prison life simply because he exercised the right to protest. A prison is never only walls and bars. It is fear, humiliation, emotional pressure, intimidation, and uncertainty. For a teenager surrounded by adult inmates, those dangers become even more alarming.
The situation becomes even more serious because Jonathan reportedly suffers from severe dyshidrosis and has previously experienced dangerous bacterial infections affecting his health. His condition requires proper medical care, hygiene, and adequate treatment, precisely the kind of stability that is difficult to guarantee inside the Cuban prison system.
Behind this story there is also a family living through a kind of pain impossible to fully describe.
Jonathan is the son of a Cuban evangelical pastor. Behind the headlines there is a mother wondering how her child is sleeping at night inside a prison cell. There is a father trying to hold onto faith while imagining the emotional and physical risks his teenage son may be facing behind bars. Faith does not erase fear. Faith does not prevent parents from trembling when their child is imprisoned.
And this is where another painful contradiction emerges.
While a Cuban pastor watches his son remain incarcerated, there are still political and religious voices outside Cuba romanticizing the Cuban regime from a safe distance. There are people who speak passionately about justice while remaining silent about political prisoners, repression, censorship, and now even the imprisonment of adolescents.
That silence matters.
Because silence protects systems that normalize abuse.
For too long, parts of the international community have spoken about Cuba through ideological nostalgia while refusing to confront the human cost paid by ordinary Cubans. The reality is not romantic. The reality is families surviving in darkness, young people fleeing the country in massive numbers, parents struggling to feed their children, and now a 16-year-old boy sitting inside a prison after joining a protest born from desperation.
No government has the moral right to destroy the emotional and psychological well-being of a teenager for exercising freedom of expression. No ideology should stand above human dignity. And no institution that claims to defend justice should remain indifferent while a child becomes a political prisoner.
Jonathan David Muir Burgos should not be in prison.
A 16-year-old boy should not have to pay for protest with his freedom.
Commentary
Complicity turned cosplay: What the Bezos-era Met Gala reveals about celebrity queerness and proximity to power
What happens when queer rebellion stops challenging power and starts posing beside it on the red carpet?
Just a few weeks ago, I went on a date with a total babe – a detail that matters less to this op-ed than I’d like, but more than Jeff Bezos’ contribution to charisma. As we approached the Metropolitan Museum of Art, we were initially greeted by a sidewalk swallowed up by white tents, the kind of scene that makes you briefly assume either a humanitarian crisis or a luxury brand activation. Thankfully, the museum was still open. While picking up tickets, the delightful woman at the counter warned us to keep an eye out for small bottles of human urine decorated with Bezos’ smooth, affectless headshot. In the most insanitary of ways, this, dare I say, performance art stunt felt like an almost too-perfect welcome for the shit show that was this year’s Bezos-adjacent Met Gala. And, in retrospect, it just may have been the most honest artistic statement the evening had to offer.
There was once a time when the Met Gala at least tried to maintain the illusion that it was about art. Yes, absurd couture has always been invited. But somewhere beneath meme-fueling lewks and masturbatory pageantry, there remained a faint institutional perfume of artistic intent. Costume as commentary, camp as critique. And now, it straight up feels less like an event of inspiring artistry and more like the world’s wealthiest tool hosting a steeply priced group project on moral dissociation. And nowhere was this contradiction more gnarly than in the enthusiastic attendance of queer-identifying celebs at the Bezos-stenched rendition of the Met Gala, a night that managed to combine the aesthetics of liberation with the spiritual energy of a Las Vegas airport lounge.
There is something uniquely bleak about watching queer public figures, many of whom built brands around marginalization and identity politics, eagerly pose beneath the glow of oligarchic patronage while much of the world appears to be freebasing social collapse. We are living through escalating global crises: genocides that many still debate and deny, gaping wealth inequality, anti-LGBTQ+ legislation, labor exploitation, housing insecurity, mass displacement, and the overarching sense that humanity casually handed the nuclear codes to a child-harming child. Yet every year, cultural elites ascend the steps of the Metropolitan Museum of Art in garments valued higher than the GDP of several municipalities while journalists whimsically gush over the trending irrelevance of it all. Read the room. Better yet, acknowledge there is a room.
What makes the spectacle particularly grating is not merely the wealth. At some point, “queerness” in elite celebrity spaces stopped functioning as a political identity and started operating more like the glam designer threads they parade at the gala, something to easily slip into and just as easily slip out of with the tides of trends, all while remaining carefully detached from the very real politics that might inconvenience proximity to power. And that is the uncomfortable contradiction exposed by events like this. If your politics evaporate in the presence of bigots and billionaires, they may not have been politics at all. They may simply have been a vibe with good lighting.
The irony, of course, is almost offensively rich. Queer art historically emerged from marginalization, criminalization, censorship, underground spaces, and collective resistance. Ballroom culture was not born because powerful institutions were benevolent patrons of expression. It emerged because excluded communities built beauty in spite of exclusion. Queer aesthetics have long transformed pain into invention, precarity into performance, and alienation into radical creativity. Now, many of those same aesthetics are repackaged as commodified luxuries for the damn near tasteless palette of the elite, detached from the social conditions that produced them to begin with. The result is a cringe caricature of culture where rebellion itself becomes purely decorative.
And this is where defenders of these spectacles usually offer the exhausted rebuttal: “Fashion is art.” You’re damn right it is, which is precisely why it cannot escape politics. Art is never apolitical because humans are never apolitical. Every artistic institution reflects systems of power: who funds culture, who accesses it, who is excluded from it, whose labor sustains it, whose suffering gets aestheticized, whose narratives become profitable. To insist otherwise is itself a political position, generally one most convenient for the already powerful.
Now more than ever, the Met Gala radiates not grandeur but desperation, specifically the desperation of elites attempting to aestheticize inequality into sophistication. Billionaires today possess astonishingly cheap taste despite astronomical wealth and resources. Perhaps because genuine taste requires curiosity, perhaps a touch of risk, and, dare I say, a degree of moral imagination. The contemporary ultra-rich have somehow made opulence feel spiritually discounted, which is why the Met reads as tacky rather than glamorous. And no, not tacky in the fun John Waters sense. Tacky in the most vapid of sense.
And queer celebrity participation matters symbolically because queer communities, historically, have often framed themselves as existing in productive tension with dominant systems of power. There was once an implicit understanding that queerness carried at least some critique of hierarchy and conformity. Now, however, one suspects the dream for many public-facing queer figures is not liberation from oppressive systems but premium seating within them. Representation alone cannot substitute for ethics.
Perhaps all of this is inevitable. Capitalism metabolizes dissent all too well. It turns subculture into branding with chilling efficiency. Punk became Hot Topic. Cornrows (not really) became “box braids” (but they tried it). Queerness became the new currency for cultural relevance. But inevitability does not make the contradiction less embarrassing, especially because the world outside these galas is anything but abstract. People are struggling materially. Many queer people, in particular, remain vulnerable economically and politically. Trans healthcare is under attack. Homophobia and authoritarian nationalism are resurging around the globe. Housing insecurity disproportionately affects LGBTQ+ youth. Workers creating the very garments celebrated on red carpets are more often than not underpaid and exploited. A concept Bezos’ Amazon employees could tell you all about, if they only had the time to.
Let’s be clear, I’m not trying to make an argument that queer public figures must retreat from culture or visibility. Visibility has always and will always matter. But visibility without conviction eventually curdles into branding. And to their credit, many queer artists and celebs have demonstrated that it is entirely possible to occupy massive platforms without surrendering political clarity in the process. Some have used award stages, interviews, performances, and social media presence to speak plainly about Palestine, anti-trans legislation, labor exploitation, racism, and the increasingly vile consolidation of wealth and power. Others have refused sponsorships, challenged institutions directly, and even donated resources under the radar. We see you, J Monaé. We see you, Acra. We see you, Mitski, Hunter Schafer, Indya Moore, Lil Nas X, Troy Sivan, and Miss Petras.
Ultimately, queer culture did not survive through assimilation alone. It survived through disruption, irreverence, solidarity, and the instinctive distrust of concentrated power wearing expensive threads. The tragedy is not that queer celebrities attend the Met Gala, it is that so many attend and remain so perfectly obedient to the systems their very queer and very dear forefathers and foremothers clapped back so hard on in the fight for basic human decency. At what point did compliance start to adorn in couture? In the end, if all else fails, you can always sneak a bottle of your own piss into the Met. It makes for a hell of a scavenger hunt.
COMMENTARY
CNN debate for California Governor: If “character matters,” where is it?
CNN California Gubernatorial Debate was on May 5, 2026

Takeaways from the CNN CA Gubernatorial debate last night. Californians are just a month shy of voting for the person who will replace Gavin Newsom as governor of this incredible, incredibly expensive, myth-producing state. But watching tonight’s debate felt a little like experiencing Eugene O’Neill’s “The Iceman Cometh” set in some old LA bar with seven characters high on their own supply going on about their “pipe dreams” with the others listening only for openings to get their digs in. What this version of the play lacked was a sober Hickey character played by Democrat Tony Thurmond to act as the moral center, someone to speak truth to the presumed power of a passionate sound bite.
Centerless, I struggled to get engaged because in this world, right now, we need our pipe dreams to live on as we madly steam into the June 2 jungle primaries. But I was taken by no one. And that’s a problem since I just got my ballot in the mail.
So here are my thoughts and observations as I do my 6 or 7 on who to vote for.
Republican Steve Hilton was given the center TV spot on stage because he has one percentage point more than Democrat Tom Steyer in the latest poll before tonight’s debate. Hilton, who is endorsed by Trump and refuses that the Donald lost the 2020 election, blamed Democrats for everything with a British accent, snide FOX TV host façade, and simplistic rhetoric designed to make people nod. The other Republican, Riverside Sheriff Chad Bianco, went from cartoonish to creepy, arrogant bully when he defended the Oath Keepers.
Low-polling Democrats Antonio Villaraigosa and Matt Mahan each had their sparkling moments but took the gloves off in attacking Xavier Becerra for knowing about a financial scandal involving his former chief of staff when Becerra was HHS Secretary. Becerra and Villaraigosa have often sparred publicly – but this was another level. “Character matters,” Villaraigosa said after calming down from a very real flash of anger.
Becerra’s response was weak, saying that if Trump’s DOJ something was there, he’d be named in the indictment too – but he’s not. He didn’t answer the “Yeah, but you knew about it” part.
This is an issue because Becerra seems to have inherited Eric Swalwell voters and jettisoned up in the polls while more and more former Biden staff colleagues said Becerra was “ineffective” in his job and would have the guts to stand up to Trump.
Katie Porter let everyone know she was behaving well onstage, even as she was virtually ignored by the TV hosts. And she got some good zingers and excellent financial points in. But while she acknowledged her leaked-video “mistake” and apologized for how she reacted to an obstinate reporter by bitching at her staff, Katie Porter’s personality transplant still only barely covered the sense that she was really an old, too-stern Mother Superior with a ruler.
Tom Steyer came off at times like a bobble-head billionaire. And while he virtually oozes authenticity, he also has an air of incredulity that some people don’t get his legit passionate commitment and sincerity. Sometimes he seems genuinely surprised that not everyone knows about his past endeavors and the Great Good motives behind them. That said, I do believe Tom Styers would know how to stand up to Trump and could even possibly pull off some deals to help the environment that no one now sees coming.
Plus, I confess – I liked Styers’ answer to who should play him in a movie. Gregory Peck, he said. He didn’t care that Peck has been dead for a long time. I think he was thinking of Gregory Peck in “To Kill a Mockingbird” – and he, too, was thinking “character matters.”
There’s another gubernatorial debate on Wednesday night on KNBC4. I’ll wait for that before I decide how I’m going to vote.
This is a cross-post from Karen’s LGBTQ+ Freedom Fighters Substack.
Commentary
How do you vote a child out of their future?
Students reportedly expelled from Eswatini schools over alleged same-sex relationships

There is something deeply unsettling about a society that turns a child’s future into a public referendum. In Eswatini, there were reports that students were expelled from school over alleged same-sex relationships, and that parents were invited to vote on whether those children should remain, forcing us to confront a difficult question on when did education stop being a right and become a favor granted by collective approval? Because this is a non-neutral vote.
A vote reflects power, prejudice and personal beliefs, which are often linked to tradition, culture, politics and religion. It is shaped by fear, by stigma, by long-standing narratives about morality and belonging. To ask parents, many of whom may already hold hostile views about LGBTIQ+ people, to decide the fate of children is not consultation. It is deferring the responsibility and repercussion. It is placing the lives of young people in the hands of those most likely to deny them protection.
And where is the law in all of this?
The Kingdom of Eswatini is not operating in a vacuum. It has a constitution that guarantees the promotion and protection of fundamental rights, including equality before the law, equal protection of the laws, and the right to dignity. The constitution further goes on to protect the rights of the child, including that a child shall not be subjected to abuse, torture or other cruel, inhuman and degrading treatment or punishment.
The Children’s Protection and Welfare Act of 2012 extends the constitution and international human rights instruments, standards and protocols on the protection, welfare, care and maintenance of children in Eswatini. The Children’s Protection and Welfare Act of 2012 promotes nondiscrimination of any child in Eswatini and says that every child must have psychosocial and mental well-being and be protected from any form of harm. The acts of this very instance place the six students prone to harm and violence. The expulsion goes against one of the mandates of this act, which stipulates that access to education is fundamental to development, therefore, taking students out of school and denying them education contradicts the law.
Eswatini is a signatory to the United Nations Convention on the Rights of the Child and the African Charter on the Rights and Welfare of the Child. These are not just commitments made to make our governments look good and appeasing. They are obligations. The Convention on the Rights of the Child is clear regarding all actions concerning children. The best interests of the child MUST be a primary consideration and NOT secondary one. According to the CRC, as indicated in the Declaration of the Rights of the Child, “the child, by reason of his physical and mental immaturity, needs special safeguards and care, including appropriate legal protection, before as well as after birth.” It is not something to be weighed against public discomfort and popularity.
The African Charter on the Rights and Welfare of the Child reinforces this, grounding rights in non-discrimination (Article 3), privacy (Article 10) and protection from all forms of torture (Article 16). Access to education (Article 11) within these frameworks is not conditional but is a foundational right. It is not something that can be taken away because a child is perceived as falling outside social norms and threatening the moral fabric of society. It is a foundational right and determines one’s ability to participate in civic actions with dignity.
So again, where is the law when children are being expelled?
It is tempting to say the law is silent but that would be too generous. The law is not silent rather, it is being ignored and bypassed in favor of systems of decision-making that make those in power comfortable. When schools and their leadership defer to parental votes rather than legal standards, they are not acting neutrally. Expelling a child from school because of allegations is not a decision to be taken lightly. It disrupts education and limits future opportunities and for children already navigating identity and social pressure, this kind of exclusion can have profound psychological effects. It isolates them. It marks them for potential harm. Imagine being a child whose future is discussed in a room where people debate your worth. That is exposure. That is harm. There is a tendency to justify these actions in the language of culture, tradition, religion and protecting social cohesion. But culture is not static and the practice of Ubuntu values is not an excuse to violate rights. If anything, the principle of Ubuntu demands the opposite of what is happening here.
Ubuntu is not about conformity. It is about recognition and is the understanding that our humanity is bound up in one another. That we are diminished when others are excluded. That care, dignity, respect and compassion are not optional extras but central to how we exist together. Where, then, is Ubuntu in a school where some children are deemed unworthy of access to education?
Why are those entrusted with protecting children are failing to do so?
There is a very loud contradiction at play. On one hand, there is a claim to shared values and to the importance of community. On the other hand, there is a willingness to isolate and exclude those who do not fit within the narrow definition of what is acceptable. You cannot have both. A community that thrives on exclusion is neither cohesive nor safe.
It is worth asking why these decisions are being made in this way. Why not follow the established legal processes? Why not ensure that any disciplinary action within schools aligns with national and international obligations? Why introduce a vote at all? The answer is uncomfortable and lies in legitimacy and accountability. A vote creates the appearance of a collective agreement. But again, I reiterate, it distributes responsibility across many hands, making it hard to hold anyone accountable. It allows the school leadership to say “lesi sincumo sebantfu”(“This is what the community decided, not me”) rather than confronting their own role in human rights violations. If the law is clear and rights, responsibilities and obligations are established, then the question is not what the community feels. The question is why those entrusted with protecting children are failing to do so.
There is also a deeper issue here about whose rights are seen as negotiable. When we talk about children, we often speak of care, of understanding, of protection and safeguarding them because they are the future. But that language becomes selective when it intersects with sexuality, particularly when it involves LGBTIQ+ identities. Suddenly, care, understanding, protection, and safeguarding give way to punishment.
Easy decisions are not always just ones.
If the kingdom is serious about its commitments under its constitution, the Convention on the Rights of the Child and the African Charter on the Rights and Welfare of the Child, then those commitments must be visible in practice, not just in policy documents. Rather, they must guide decision-making in schools and in communities. That means recognizing that a child’s right to education cannot be overridden by a show of hands. It means ensuring that schools remain spaces of inclusion rather than sites of moral policing. It means holding leaders and institutions accountable when they fail to protect those in their care.
Bradley Fortuin is a consultant at the Southern Africa Litigation Center and a human rights activist.
COMMENTARY
Is the Stonewall Generation being screwed by the San Diego LGBT Center?
Seniors question the handling of an $18.9 million bequest intended to support them

Beautiful San Diego, the second largest city in California, is shuddering through challenging times. Amid city deficits, federal budget cuts and emotional and fiscal consternation over the war in Iran, the LGBTQ+ community is facing, what to some, is an ego-driven tiff and, to others, is a deep dispute over transparency and trust between the San Diego LGBT Community Center and Stonewall Generation seniors who want to know what’s happening with an $18.9 million gift their late friends bequeathed the Center for senior services, programs, and housing.
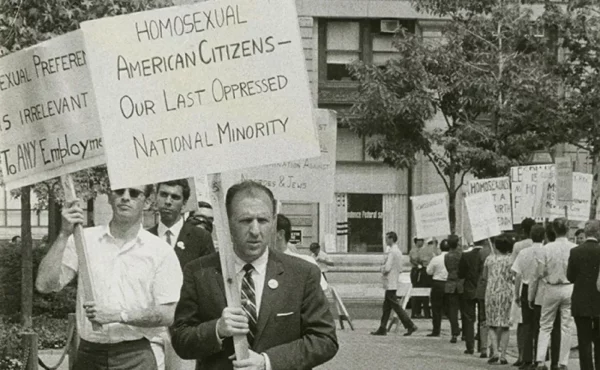
While this may seem like some niche soap opera that will blow over with enough delay, the circumstances are darker and more dire than the drama reveals. On the surface, exchanges between the two camps appear politely professional. But there is a deep, widening, and hardening chasm developing between those who fought for gay liberation when homosexuality was still a criminal perversion, and the Center board and staff committed to protecting vulnerable LGBTQ+ youth who only know Trumpian cacophony in a nihilistic world.
The feud is growing so loud that it is drowning out the fiscal winds banging outside the Center door, harbingers of massive tornadoes threatening to obliterate the house. The “what ifs” are near: what if government funding is cut to the quick and donors start questioning their once-firm trust in Center management?
Particularly painful: a source overheard some Center youth dismiss the Stonewall Generation seniors: “They’re just bitter old racist cis queens causing all the trouble.” What happens if a significant number of gay white men act on what is now just a whispered feeling: “Why should I care about the Center? They hate us!”
Who’s going to fund the Center without an engaged and unified community?
The terrible irony is that without recognition of the stakes and the need for authentic negotiation, the feud may render the Center complicit in Project 2025’s erasure of LGBTQ+ people.

Context: The Gathering Storm
San Diego was once a bastion of conservative Republicanism, but its political landscape has skewed blue over the past two decades, led in part by trailblazing out lesbian political icons Christine Kehoe and Toni Atkins, who paved the way for Todd Gloria to become the first out LGBTQ+ person and the first person of color to serve as the city’s mayor.
But with the historic honor comes grave responsibility, including Gloria’s proposed $2.2 billion budget for the new fiscal year with significant cuts to close a projected $146 million deficit. “Find the money elsewhere,” protesters at City Hall screamed at a Monday night meeting on April 20th.
In early April, Trump revealed his full discretionary budget request for fiscal year 2027 – obviously not including expected requests for the Department of Homeland Security in the aftermath of the incident at the White House Correspondents Association dinner. The budget would reduce nondefense discretionary spending by $73 billion, including $33.5 billion in funding cuts for the Department of Housing and Urban Development (HUD), according to a bipartisan policy analysis.
Despite promises not to cut safety net programs — and an added $174 million in prospective renovations to his $400 million gilded ballroom — Trump later said it’s “not possible” for the federal government to fund Medicare, Medicaid, and child care costs, adding that the states should “take care” of those programs while the federal government focuses on the military. The food assistance program SNAP has already dropped 2.5 million people.
Steve Rattner, a prominent economic analyst, told MS NOW that Trump’s proposed budget is a reincarnation of Project 2025. If passed, the budget would be the most dramatic re-structuring of federal government spending “since certainly the New Deal and who knows when beyond that.”
The proposed cuts are real, deep, wide, and cultural. Preparing for America’s 250th anniversary, Trump issued Executive Order 14253, Restoring Truth and Sanity to American History and ordered a sweep of the Smithsonian Institution: “Museums should begin implementing content corrections where necessary, replacing divisive or ideologically driven language with unifying, historically accurate, and constructive descriptions across placards, wall didactics, digital displays, and other public-facing materials.” Historic narratives to be “corrected” include exhibits about slavery, the violent Manifest Destiny ruination of Indigenous people and the relatively new recognition of LGBTQ+ history.

But not all anti-LGBTQ+ cultural attacks are happening behind closed doors. Last year, San Diego woke up to the Union-Tribune headline: “Chucky Lozano’s injury, homophobic chant temper San Diego FC’s soccer celebration.” SDFC coach Mike Varas decried the one-word chant as “palabras discriminatorias” or “discriminatory language.”
The infamous homophobic soccer chant recently resurfaced in Mexico, which is co-hosting the 2026 World Cup with the US and Canada. FIFA has scheduled eight matches this summer in LA’s SoFi Stadium, including the highly coveted U.S. Men’s National Team (USMNT) opening match. Think security and Border Patrol will care about a little sports-related gay-bashing during Pride season?
Violence is in the air, with winds picking up speed, veering toward the vulnerable.
The Feud, in Summary
The San Diego LGBT Center is aware of the pending fiscal crisis. On July 3, 2025, the Center issued an urgent preemptive warning to its 106 employees of possible layoffs around Sept. 6 in anticipation of federal cuts. Center spokesperson Gus Hernandez told the San Diego Union-Tribune that about $4.4 million of the Center’s $15.5 million budget comes from federal grants from HUD and the Department of Health and Human Services (HHS).
“It’s very precarious right now with the federal funding,” Hernandez said. “We’re not putting on rose-colored glasses … We think it will happen to us.”
It didn’t. There were no layoffs. The Union-Tribune noted the Center’s growth from 63 employees and a budget under $5 million in 2015 to 106 on staff and more than $15 million in July 2025.
“The nonprofit’s tax filings have been audited every year since 2011, and from 2021 to 2023, the audits found repeated deficiencies in The Center’s financial reporting. The Center’s most recent audit, for the fiscal year ending June 2024, came back without any concerns,” the Union-Tribune reported. “The Center did not immediately respond to questions about why it took so long to correct the deficiencies, but Hernandez blamed the problems on rapid and unexpected growth at the Center.”
“We’ve been growing a little bit faster than we anticipated,” Hernandez said. “Every year, we’ve just been growing and growing and adding programs and adding services. And I think in that growth process … we weren’t keeping up our accounting to match that growth.”
A handful of Stonewall Generation seniors pressed the Center board for a more complete and thorough explanation of why their published Financial Statements and Annual Reports from 2021 to 2023 show changing descriptions of what the seniors assume is the $18.9 million gift from the estate of Maurice Thimot and M. Rust Rawnsley.
On Tuesday, April 21, Ted Callam, Charles “Chuck” Kaminski, and Elaine Lewis of Pride Across Generations and 120 community supporters issued a press release calling for attendance at the Center board meeting on Tuesday, April 28, 6:30 PM at the Center Auditorium. They said Note 15 in the Center’s 2025 audit “raises serious questions.”
The audit “shows that nearly $1 million was reclassified as donor-restricted — retroactively to 2023,” they reported. “In plain terms: funds previously treated as unrestricted are now being acknowledged as restricted all along. The amount closely matches the annual income associated with the Thimot–Rawnsley Fund bequest.”
And that, they said, “creates urgent questions for the community,” including “Who is advising these decisions on behalf of our community?”
“This is not about speculation. It is about transparency, accountability, and honoring donor intent. The stakes reach beyond one fund. This affects trust in the Center and confidence across San Diego’s senior LGBTQ+ community,” they said. “We are not asking for more. We are asking for clear answers — and for what was already meant for our community.”
The board responded two days later, via an April 23 email from longtime Center board member Sue Reynolds, who thanked the leaders for their letter and promised to pass it along to the board treasurer and the rest of the board. She then noted the message attached at the end of a promotion for the Dining Out for Life event held that night, which “responds to the questions/issues you posed.”
Here’s the Center’s message:
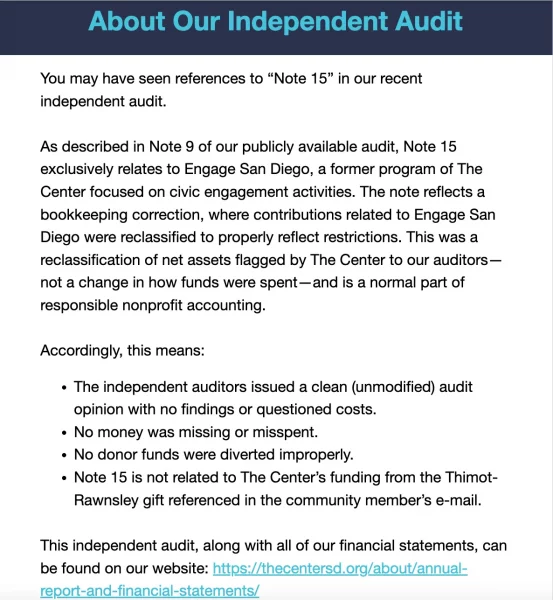
The Center closed with a promise to be transparent:
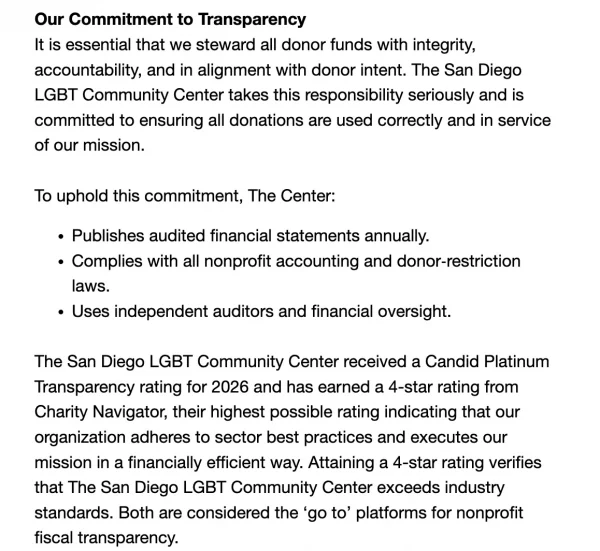
And herein lies the crux of the feud.
The Center may be transparent with the government and general public about its numbers, but these Stonewall Generation retired professionals – who are not accountants – are transparently honest and quick to fix a misconception.
“In our previous email, we pointed out Note 15 in the 2025 audit report. The Center clarified that the Note refers to another Center program and not to the Thimot Rawnsley Fund. If only the Center would respond as rapidly and as clearly with regard to the Fund questions we have asked them, we would then expect these issues raised to be resolved,” Kaminski wrote to supporters Sunday night.
The Stonewall Seniors have been asking about the donation since Center CEO Cara Dessert first announced it in the Center’s June 13, 2022, newsletter.
“This amazing couple has created a legacy for our community’s future, directing The Center to establish a fund, The Maurice J. Thimot and M. Rust Rawnsley Fund (the Thimot and Rawnsley Fund). The purpose of the Thimot and Rawnsley Fund includes investing in our LGBTQ seniors. We look forward to stewarding this fund by investing in our senior services, exploring long-term investments in capital projects, and soliciting feedback from our community,” Dessert wrote.
“Once we have a full understanding of the fund and any proceeds from the fund itself, we look forward to sharing more with our Center community and seeking input about our future!” she continued. “We are deeply grateful to Rust and Maurice for their confidence in The Center, their generosity, and their care for our San Diego LGBTQ community, especially our seniors. Stay tuned for more information about the Thimot and Rawnsley Fund at The Center!”
The Stonewall Seniors expected their input to be solicited and questions answered such as: could the $18.9 million and the interest it generates be used for something other than senior housing and programs, as the late gay couple had often publicly discussed? In the March 31, 1990 issue of Update discussing SAGE, for instance, Maurice J. Thimot specifically talked about housing.
There’s also precedent. When Dr. Delores Jacobs announced her retirement as the Center’s chief executive in June 2018, for instance, “more than 200 interviews and focus groups, [and] feedback was solicited regarding characteristics sought in the new Center chief executive, led by Board Co-Chair Joyce Rowland,” the Center announced.
The Stonewall Seniors say the Center has given varied explanations about the gift, the first $10 million of which came in 2022, the remainder in 2024, and they want to see the language of the Thimot-Rawnsley estate trust to find out how their bequest was to be used.
“It’s four years of interpretations, four years of shifting explanations, four years of telling this community to trust them without ever producing the one document that would actually answer the question,” said Ted Callam, who served on the Center’s senior advisory committee before it was disbanded and replaced with new members.
Center officials initially said the gift would be used for community programs and spaces with an emphasis on seniors. There was also talk of expanding the building, according to Callam, Kaminski, and Lewis. But that did not come to fruition. Then, last December, Center leaders said the gift was restricted to seniors, housing, and housing-related services and could not be used to establish a senior center.
Earlier, the Center’s board of directors had approved an annual draw of $350,000 from the bequest to fund housing navigation, rental assistance, and eviction prevention. Center officials further said interest income may be used for certain interconnected services, on the basis that seniors are part of everything the group does. But now the $350,000 draw has been paused until the Center hears from its attorneys and consultants.
In a recent newsletter, Center officials said they are “awaiting final guidance and will continue providing transparent, quarterly updates, with our next update scheduled for this summer.”
“We’ve watched the story change,” Callam said. “So senior programs and services, then senior housing, then housing and related services, and now ‘we’re awaiting guidance.’”
At the Center’s March 24 board meeting, several seniors spoke up, including Tom Kirkman, who ran San Diego’s SAGE Center from 2000 to 2009, when Thimot was on the board of that organization.
“Maurice and Rusty were very interested in the quality of life for seniors,” Kirkman told LGBTQ Freedom Fighters. He believes they would have wanted their bequest to support senior services, although he hasn’t seen whatever document governs that. “I’m looking forward to seeing that document,” he said. (San Diego’s SAGE organization, now disbanded, was independent and not affiliated with the national group of the same name.)
LGBTQ+ seniors initially offered to help the Center decide how to spend the bequest, Lewis said. “They said, ‘Yes, we want the community involved. Yes, we’re going to talk to the community,” she recalled.
Both Lewis and Callam have experience in designing surveys, and they decided to create one, only to find that the Center had sent one out already. That survey was useless because it didn’t ask if respondents were part of the LGBTQ+ community, she said.
Kaminski has filed three ethics complaints with the California attorney general’s office over the handling of the bequest. A staff member responded that the AG’s office does not have the resources to investigate every complaint filed and that it does not investigate certain types of complaints. The staffer also told Kaminski that the AG does not comment on ongoing or potential investigations, which was the same answer LGBTQ Freedom Fighters received.
As for the legalities concerning the Center’s use of the funds: If there are written restrictions on a donation’s use, the terms are legally binding. Only the donors, not the recipient, can impose such restrictions. But the terms do not have to be shared publicly, according to the National Council of Nonprofits.
“Because this was a complex, multi‑property estate, we conducted an extensive, multi‑year due diligence process with legal and accounting specialists. We are implementing a clear strategy that strengthens current services benefiting LGBTQ+ seniors while ensuring long‑term organizational stability and compliance with donor intent,” Center spokesperson Hernandez said.
“Over the last nearly four years, The Center conducted a careful, thorough review of the $18.9 million bequest, which was received in full in September 2024. This review included monitoring the progress of the sale of 21 domestic and international properties and consultations with multiple specialists, who at times had differing opinions on the scope of the bequest’s intent,” he continued.
“To ensure that this extraordinary gift is used in the way it was intended, we assembled a team of experts that includes our attorneys and auditor. It took time to organize the team and for them to align on how the full gift could be utilized to maximize the benefit to the community. As we near the end of this long process, we are awaiting final guidance to ensure our shared interpretation follows all regulations related to charitable assets. We have paused the use of gift funds until that final guidance is confirmed,” Hernandez said.
The Center gave a similar answer to Manuel Reyes, an aide to San Diego City Council member Jennifer Campbell, who represents the district where the center is located. Callam, Kaminski, and Lewis did not find the answer satisfactory.
In a letter to Reyes and Campbell, they emphasized that the Center should release the original bequest language and questioned why, if the bequest required interpretation, it had taken so long. They also wondered if the funds had been used for purposes other than the donors intended.
Lewis, Callam, and Kaminski of Pride Across Generations said the Center has disrespected seniors in other ways. There used to be a drop-in room dedicated to seniors. “It was the perfect room, because it has an outside entrance, and there were always seniors in there, and there were snacks and conversation, and if somebody needed help, they could go in and ask,” Lewis said. But it was turned into an office, and senior resources were moved into a hallway off the library, which was inaccessible because of meetings in the library, and “even to get past the front desk, you had to ask permission and have some reason to be there,” she said.
The disbanding and replacement of the senior advisory committee is another sore point with the three. Center officials said they wanted a new model, but someone with the Center did comment that the earlier committee was “too white and too cisgender.” The new committee’s members and meeting dates are not made public, according to Kaminski, Lewis, and Callam. How do you get community information to a multi-layered secret committee, and how do you find out results?
“I have served on the boards of many nonprofits over nearly 50 years and I have never seen anything like this,” says out former KNBC4 reporter Garrett Glaser, who signed the Pride Generations’ March 15 letter to the Center board and senior leadership.
That letter says, in part: “When seniors ask questions about governance, finances, and mission alignment, they are not being disruptive—they are exercising their right to understand how an organization that claims to serve them is being run. Treating those questions as something to be managed or silenced undermines trust and excludes the very community the Center exists to support.
“Trust and transparency are earned through consistent integrity, not rhetoric. Until the Center demonstrates genuine accountability, transparency, and meaningful engagement with LGBTQ+ seniors, trust remains broken.”
So, who is asking what happens if and when that fiscal tornado hits?
Pride Across Generations requests your presence and possible participation in the Center’s board meeting on Tuesday, April 28 at 6:30 PM in the Center Auditorium. The theme: “Honor the Past. Secure the Future. Moments like this define institutions. Let’s show up—for transparency, accountability, and trust.”
The meeting will also be available on Zoom.
You can reach Pride Across Generations at: [email protected]
This is a cross-post from Karen’s LGBTQ+ Freedom Fighters Substack.
Commentary
Is Trump setting a trap for White House journalists at their big dinner?
White House Correspondents Association must do something to honor the free press

The old order is gone. Donald Trump didn’t just upset the apple cart of traditional rules and propriety – he set it on fire and laughed as his sycophants ushered his retreat into a fantasy gilded castle where he can be king for life.
Even beloved former First Lady Michelle Obama set aside her famous “we go high” approach to morally withered Republicans and, in the face of the obvious dangers to democracy Trump presented, urged Democrats to get politically practical before the 2024 elections.
“If we start feeling tired, if we start feeling that dread creeping back in, we’ve got to pick ourselves up, throw water on our faces, and do something,” Obama said.
Do something.
The grassroots chorus from “We the People” has grown louder and louder since regular, ordinary people took to the freezing, snow-covered streets of Minneapolis to protest the killing of two American citizens trying to protect their immigrant neighbors from militarized ICE agents. Recently, momentum from the massive No Kings rallies has shifted to local, regional, and state races as the critical midterm elections approach, and Democrats have been largely successful in their new “fight fire with fire” strategy.
But Trump seems obsessed with building his $400 million ballroom instead of doing something to help Republicans win elections, including sitting on an unspent $500 million war chest, while, as Alternet notes, his popularity steadily declines among once fierce loyalists.
“Even Fox News is now reporting Trump’s approval rating has plummeted to 33 percent [AP/NORC poll] over his foolish decision to send the US economy into a likely recession over his decision to fight an unnecessary and unprovoked war of aggression,” wrote David Pyne, a former America First Trump supporter and security expert who serves as a Deputy Director of National Operations for the Task Force on National and Homeland Security.

Meanwhile, Trump continues to stick it to the media, which he describes as the “enemy of the people.” That group now includes former conservative allies like Tucker Carlson, Megyn Kelly, Candace Owens, and Alex Jones, who he describes as “nut jobs” and “troublemakers” for criticizing him over the still-unexplained war in Iran.
Trump likes using his power to humiliate – especially women journalists of color – and retaliate against his enemies, a key tenet of the Authoritarian Playbook that organizations like Protect Democracy continue to update and explain.
“I say up front, openly, and proudly, that when I WIN the Presidency of the United States, they and others of the LameStream Media will be thoroughly scrutinized for their knowingly dishonest and corrupt coverage of people, things, and events. Why should NBC, or any other of the corrupt & dishonest media companies, be entitled to use the very valuable Airwaves of the USA, FREE? They are a true threat to Democracy and are, in fact, THE ENEMY OF THE PEOPLE! The Fake News Media should pay a big price for what they have done to our once great Country!” Trump’s post on Truth Social, Sept. 2023, before winning a second term in 2024.
The Authoritarian Playbook for 2025 explains: “A hallmark of any democracy is the freedom to criticize the government without fear of censorship or reprisal. Trump has promised — and has developed plans — to use the regulatory and administrative powers of government to force political loyalty; sow disinformation; and quash speech by journalists and media outlets, businesses, and other private citizens. These plans follow the measures used by Viktor Orbán in Hungary and other 21st-century autocrats to transform government power to serve the parochial interests of the ruler, not the broader public.”
Despite Trump’s support, Orban recently lost re-election, ending 16 years of “electoral autocracy.”
Trump and his administration also expanded attacks on the First Amendment, with the FBI investigating a New York Times reporter who wrote about the director Kash Patel using taxpayer-funded bureau personnel and resources to provide security for his girlfriend. The investigation included searching databases for information on reporter Elizabeth Williamson to see if she broke any federal stalking laws.
“The F.B.I.’s attempt to criminalize routine reporting is a blatant violation of Elizabeth’s First Amendment rights and another attempt by this administration to prevent journalists from scrutinizing its actions,” said Joseph Kahn, the executive editor of The Times. “It’s alarming. It’s unconstitutional. And it’s wrong.”
Interestingly, news of the Justice Department’s apparent retaliatory action leaked days before the White House Correspondents Association (WHCA) dinner on Saturday night, April 28. Trump’s acknowledgement of the WHCA invitation is like an obnoxious little boy sticking his tongue out.
“The White House Correspondents Association has asked me, very nicely, to be the Honoree at this year’s Dinner, a long and storied tradition since it began in 1924, under then President Calvin Coolidge. In honor of our Nation’s 250th Birthday, and the fact that these “Correspondents” now admit that I am truly one of the Greatest Presidents in the History of our Country, the G.O.A.T., according to many, it will be my Honor to accept their invitation, and work to make it the GREATEST, HOTTEST, and MOST SPECTACULAR DINNER, OF ANY KIND, EVER! Because the Press was extraordinarily bad to me, FAKE NEWS ALL, right from the beginning of my First Term, I boycotted the event, and never went as Honoree. However, I look forward to being with everyone this year. Hopefully, it will be something very Special. Thank you for your attention to this matter! President DONALD J. TRUMP,” he posted March 2 on Truth Social.
Some enraged journalists called for the fundraising dinner to be cancelled. Veteran ABC News journalists Ian Cameron and Lisa Stark had another idea: get colleagues to sign a public letter to WHCA urging them to do something to protest Trump’s authoritarian tactics.
“We first began thinking about this in late March, as it became clear the President would attend the dinner. We just felt we had to speak out about this,” former ABC News correspondent Lisa Stark told LGBTQ+ Freedom Fighters. “The WHCA dinner is held to celebrate the First Amendment and freedom of the press, and yet the guest of honor is the man who, along with his administration, has done everything possible to undermine freedom of the press and destroy trust in the press.”
The response has been overwhelming. After several days of outreach, the ad hoc group collected 414 signatures (including mine as a former journalist for CBS News/LGBTQ press), as well as six press/First Amendment organizations.
“It’s gratifying that so many former journalists see a threat to press freedom and want to speak out,” says Stark. “We know current journalists, those in the media trenches now, aren’t in a position to raise their voices. We feel an obligation to do so on their behalf. We can’t treat this as business as usual – these are not normal times.”
The petition cites 22 instances of Trump’s attacks on the press and First Amendment, not including the most recent involving the NY Times and updates on the Associated Press lawsuit.
“The collective weight of the administration’s actions — retaliatory access bans, coercive regulatory investigations, frivolous lawsuits against the press, defunding of public broadcasting, dismantling of international broadcasting, physical restrictions on journalists, personal verbal attacks on reporters, assaults on the media in official White House press releases and social media posts, the arrest of journalists, and the pardoning of those who committed violence against the press — represent the most systematic and comprehensive assault on freedom of the press by a sitting American president,” the petition reads, in part.
“We understand that some journalists plan to wear pocket handkerchiefs or lapel pins with the words of the First Amendment,” the petition says. “And continuing in that spirit, we believe the White House Correspondents Association should take stronger action by issuing – from the podium – a forceful defense of freedom of the press and condemnation of those who threaten that freedom, followed by a standing toast to the First Amendment and a pledge to continue upholding such a critical cornerstone of our democracy. Speak forcefully, in front of the man who seeks to undermine our country’s long tradition of an independent, strong, and free press.”
The petition concludes: “We also urge the WHCA to reaffirm, without equivocation, that freedom of the press is not a partisan issue and that the Association will not normalize this behavior but instead fight back against any officeholder who has waged systematic war against the journalists whose work the dinner celebrates.”
What now? The Daily Beast reports that “Donald Trump will launch a ‘revenge’ attack on the White House media when he confronts them in person at a Washington dinner on Saturday night—then flee before there can be revenge.”
Might the WHCA DJ play him off stage with Roy Orbison’s “Running Scared?”
But Trump will have cronies in the room who will turn his antics into memes about “crushing” the “lamestream media.” It’s an obvious ploy to excite Trump’s base.
In a scathing column, longtime journalist Margaret Sullivan notes that some media companies and bosses have gone from courtesy to courting, “inviting blatantly anti-press officials, including the defense secretary, Pete Hegseth, and the White House deputy chief of staff, Stephen Miller, to be guests at their tables, or (in the case of David Ellison, CEO of CBS News’s parent company) even holding a separate dinner to “honor” Trump. Paramount, the parent of CBS News, is said to have invited Brendan Carr to their table; he is the FCC chair who has made a mockery of what should be his independent and non-partisan role; appointed by Trump, he has come down clearly on the side of the president’s allies in consequential decisions – including those involving Paramount’s mergers with other media corporations.”
“It’s akin to a fire department inviting arsonists to a gathering aimed at celebrating firefighting,” Sullivan quotes Oliver Darcy as writing in his media newsletter, Status.
So, gala attendees, as the petition asks, Please Do Something!
This is all particularly jarring for LGBTQ+ journalists. Eric Schultz was the first out gay deputy White House press secretary to give briefings during the Obama administration. Then came the first Black lesbian, Karine Jean-Pierre, during the Biden administration, and the independent WHCA assigned a seat (shared with the Boston Globe) and rotating pool responsibilities to the LGBTQ+ Washington Blade, which still retains the privilege.
But for those of us who remember President Reagan’s Press Secretary Larry Speakes laughing and ridiculing White House reporters when he was asked about Reagan’s position on AIDS, being officially seated was a big deal. When CSPAN started broadcasting the dinner in 1993, we scanned every TV inch to see who might be wearing Red Ribbons to the “Nerd Prom,” who might be gay, and who we knew to be closeted – spinning President Clinton’s anti-gay Don’t Ask, Don’t Tell policy to favor anti-gay Democratic Sen. Sam Nunn.
And then there was the “Golden Age,” as the Washington Post described the gala in 2023. “There was the time Ellen DeGeneres, just days out of the closet, canoodled with new girlfriend Anne Heche right in front of Bill Clinton. The time George W. Bush goofed around with a George W. Bush impersonator. The time Barack Obama dunked on reality TV star Donald Trump to the rapturous shrieks of the media elite. What a time to be alive, and in attendance, at the White House Correspondents’ Association dinner!”
Last year, post-COVID, WHCA was headed by married Black gay Eugene Daniels, MSNBC’s Senior Washington Correspondent. The stars were the parade of journalists of color, mostly women, who served as co-hosts, presenters, honorees, and award winners.
Daniels addressed the missing orange man in the room. “We don’t only extend invites to the presidents who say they love journalists or who say they’re defenders of the First Amendment and a free press. We invite them to remind them that they should be,” Daniels said.
“When Thomas Jefferson wrote in 1786 that, ‘Our liberty depends on the freedom of the press and that cannot be limited without being lost,’ he and the other framers of the United States understood the danger unchecked power poses to the ideals and people of this nation,” he continued.
“We journalists are a lot of things,” Eugene Daniels said last year to a ballroom of 2,600 attendees. “What we are not is the enemy of the people, and what we are not is the enemy of the state….Every single day, journalists in this country face threats of intimidation, lawsuits, and violence. Those attacks are meant to do one thing: stop us from sharing the truth with the people…
“I want to leave you with the words of a trailblazing journalist, Ida B. Wells, ‘The way to right wrongs is to turn the light of truth upon them.’ Despite everything, I’m still optimistic about the power of what we do and more assured than ever of the importance of defending it. Everyone in this room can and should stand in the breach. Everyone can and should push for what we know is right. Everyone can and should stand up against government interference in a free press. And a promise I make to you is that the White House Correspondents Association, this board, will always defend your right to do your jobs.”
We’ll be watching CSPAN. Show us you mean it. Do something!
Read the full petition with signatories here.
This is a cross-post from Karen’s LGBTQ+ Freedom Fighters Substack.
Eight Democrats break with party as House advances ‘Don’t Say Trans’ bill

Why fans ‘complete’ the Storrie: The psychology behind RPF & fandom narratives

Iran war causes condom shortage in India

Politicians, activists pay tribute to Barney Frank

U.S. attorney nominee confirmed despite anti-LGBTQ+ history, no trial experience

Texas Children’s Hospital reaches $10 million settlement with DOJ over gender-affirming care

Intersex lives, constitutional freedom, and the dangerous future of Ghana’s Human Sexual Rights and Family Values Bill

Anti-LGBTQ+ commentator Tyler O’Neil to testify in Southern Poverty Law Center probe

Cuba marks IDAHOBiT amid heightened tensions with U.S.

BREAKING NEWS: Barney Frank dies at 86
-
 Federal Government3 days ago
Federal Government3 days agoTexas Children’s Hospital reaches $10 million settlement with DOJ over gender-affirming care
-
 Ghana2 days ago
Ghana2 days agoIntersex lives, constitutional freedom, and the dangerous future of Ghana’s Human Sexual Rights and Family Values Bill
-
 Congress3 days ago
Congress3 days agoAnti-LGBTQ+ commentator Tyler O’Neil to testify in Southern Poverty Law Center probe
-
 Cuba4 days ago
Cuba4 days agoCuba marks IDAHOBiT amid heightened tensions with U.S.
-
 National2 days ago
National2 days agoBREAKING NEWS: Barney Frank dies at 86
-

 a&e features4 days ago
a&e features4 days agoThe 40th anniversary of ‘Pee-wee’s Playhouse’ was a celebration of weird, queer art
-
 AIDS and HIV4 days ago
AIDS and HIV4 days agoSB 1023 takes aim at the invisible insurance barriers to HIV prevention
-
 Wyoming2 days ago
Wyoming2 days agoU.S. attorney nominee confirmed despite anti-LGBTQ+ history, no trial experience
-

 Features2 days ago
Features2 days agoFrom above our heads to underneath our steps: Lynn Segerblom’s ongoing journey of Pride through public art
-

 Vermont2 days ago
Vermont2 days agoVt. lawmaker equates transgender identity with bestiality